Clear Sky Science · en
Adherence to international neural monitoring study group (INMSG) guidelines for intraoperative nerve monitoring in thyroid and parathyroid surgery. A survey of endocrine surgeons in Spain
Why this matters for your voice
Thyroid and parathyroid surgery takes place in a crowded space in the neck, right next to the tiny nerves that move the vocal cords. If those nerves are hurt, people can be left with hoarseness, trouble speaking, or even breathing problems. A technology called intraoperative nerve monitoring acts like a “nerve alarm” during surgery, helping surgeons see how these nerves are doing in real time. This study asked endocrine surgeons across Spain how closely they actually follow international recommendations for using this technology, and what they think about it.
The nerve at the heart of speech
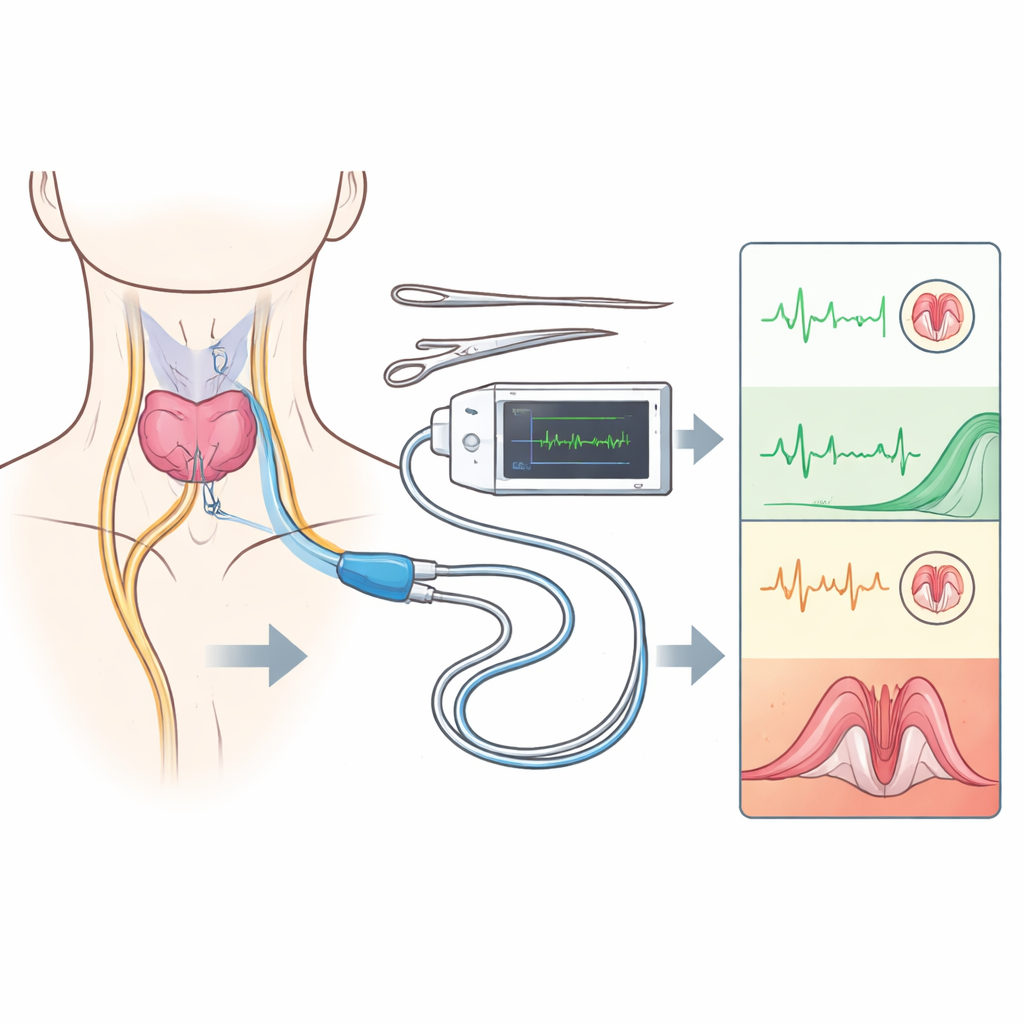
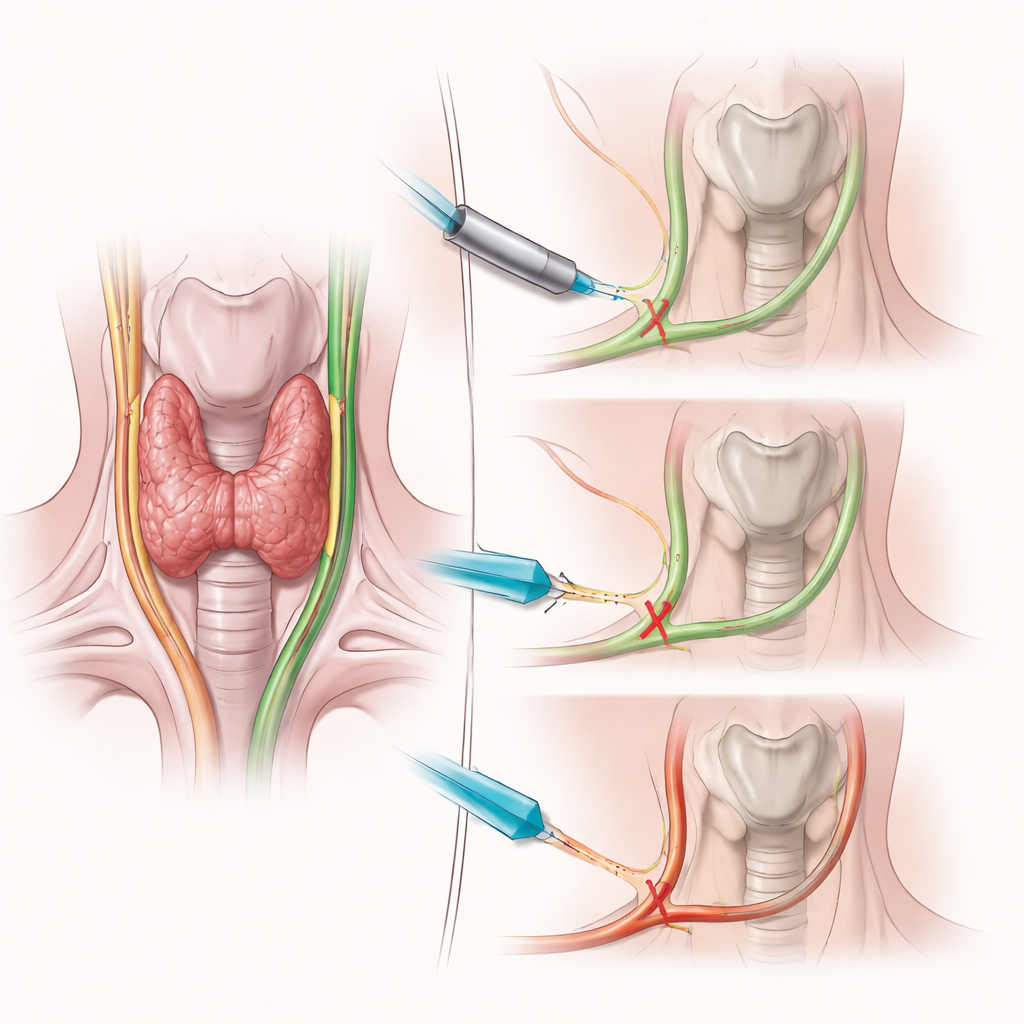
The key player in this story is the recurrent laryngeal nerve, which controls the vocal cords. Damage to it, even though relatively uncommon, can seriously affect quality of life. Surgeons can usually see the nerve during an operation, but sight alone does not reveal whether it is still working. Intraoperative nerve monitoring adds a kind of electrical “stethoscope” for the nerve, giving an immediate signal when function changes. International expert groups have developed detailed step‑by‑step routines and safety rules for when and how to stimulate the nerve and how to react if the signal is lost. These rules are meant to make surgery safer and to reduce lifelong voice problems.
A nationwide look inside the operating room
To understand how these rules are used in real life, the researchers sent an anonymous online questionnaire to 719 endocrine surgeons who belong to the Spanish Association of Surgery. The survey, available for seven months in 2021, gathered complete responses from 112 surgeons. Questions covered three main areas: how well surgeons followed international procedures during operations; what they believed about the usefulness, safety, and legal value of nerve monitoring; and how they and their trainees learn to use the technology. The answers paint a detailed picture of a health system where nerve monitoring is widely accepted in principle but unevenly applied in practice.
Guidelines on paper versus habits in practice
Most respondents—about four out of five—said they follow the recommended sequence of nerve checks during surgery. Yet when the survey probed specific steps, gaps appeared. Only about half of surgeons routinely stimulated the vagus nerve at the beginning of the operation, and even fewer did so at the end, despite this being a cornerstone of the international protocol. Many surgeons were unsure of the exact electrical thresholds that signal real danger for the nerve, and more than a third did not clearly distinguish between localized and widespread types of signal loss—information that should guide whether to stop and stage the surgery to avoid paralysis on both sides. Just over half said they followed the official troubleshooting algorithm when the signal disappears, and many would still push ahead with full thyroid removal for cancer even after a confirmed signal loss on the first side.
Patients informed less than technology suggests
The survey also explored what surgeons tell patients and how they view legal responsibilities. Fewer than half consistently informed patients before surgery that nerve monitoring would be used and what that might mean. Only a tiny minority—about one in twenty—used a specific written consent form for this technology, even though many surgeons believed that monitoring offers legal protection and helps document that best efforts were made to protect the nerve. Most respondents felt nerve monitoring boosts their confidence, helps prevent nerve injury, and is particularly valuable for training young surgeons. At the same time, opinions were split on whether it truly reduces costs or should be considered an absolute requirement for every thyroid or parathyroid operation.
Training the next generation
Nearly all of the surgeons worked in units that train residents, and almost all agreed that nerve monitoring is helpful for learning. Many had attended courses or scientific meetings about the technology and rated their own expertise as advanced. Yet their answers about practical steps—such as how often they stimulate the vagus nerve or how they respond to loss of signal—suggest that some of this confidence may be misplaced. The authors argue that better‑structured training, with hands‑on practice and clear teaching on how to interpret signal changes, is needed so that surgeons do not misuse or overtrust the equipment.
What this study means for surgical safety
For patients, the takeaway is that nerve monitoring is widely used and generally valued by surgeons, but its most protective features are not always applied consistently, and conversations about it before surgery are often incomplete. The authors conclude that stronger education, clearer patient information, and dedicated consent for nerve monitoring are essential if this technology is to fulfill its promise: fewer damaged voice nerves, safer thyroid and parathyroid operations, and more reliable evidence on what truly works in the operating room.
Citation: Durán-Poveda, M., Vidal Pérez, O., Martos Martínez, J.M. et al. Adherence to international neural monitoring study group (INMSG) guidelines for intraoperative nerve monitoring in thyroid and parathyroid surgery. A survey of endocrine surgeons in Spain. Sci Rep 16, 13499 (2026). https://doi.org/10.1038/s41598-026-43651-0
Keywords: thyroid surgery, nerve monitoring, voice nerve injury, surgical safety, surgeon training