Clear Sky Science · en
Modelled impact of a multi-cancer early detection screening programme on the demand for diagnostics in England
Why this matters for everyday health care
Imagine a single blood test that can flag signals for dozens of different cancers long before symptoms appear. That is the promise of multi-cancer early detection (MCED) tests. But if many more people are told they might have cancer, health systems must be ready with scans, scopes, and biopsies to confirm who is really ill. This study asks a simple but crucial question for England’s National Health Service (NHS): if such a test were rolled out nationally, how much extra strain would it put on already busy diagnostic services?
How a single blood test could change the care pathway
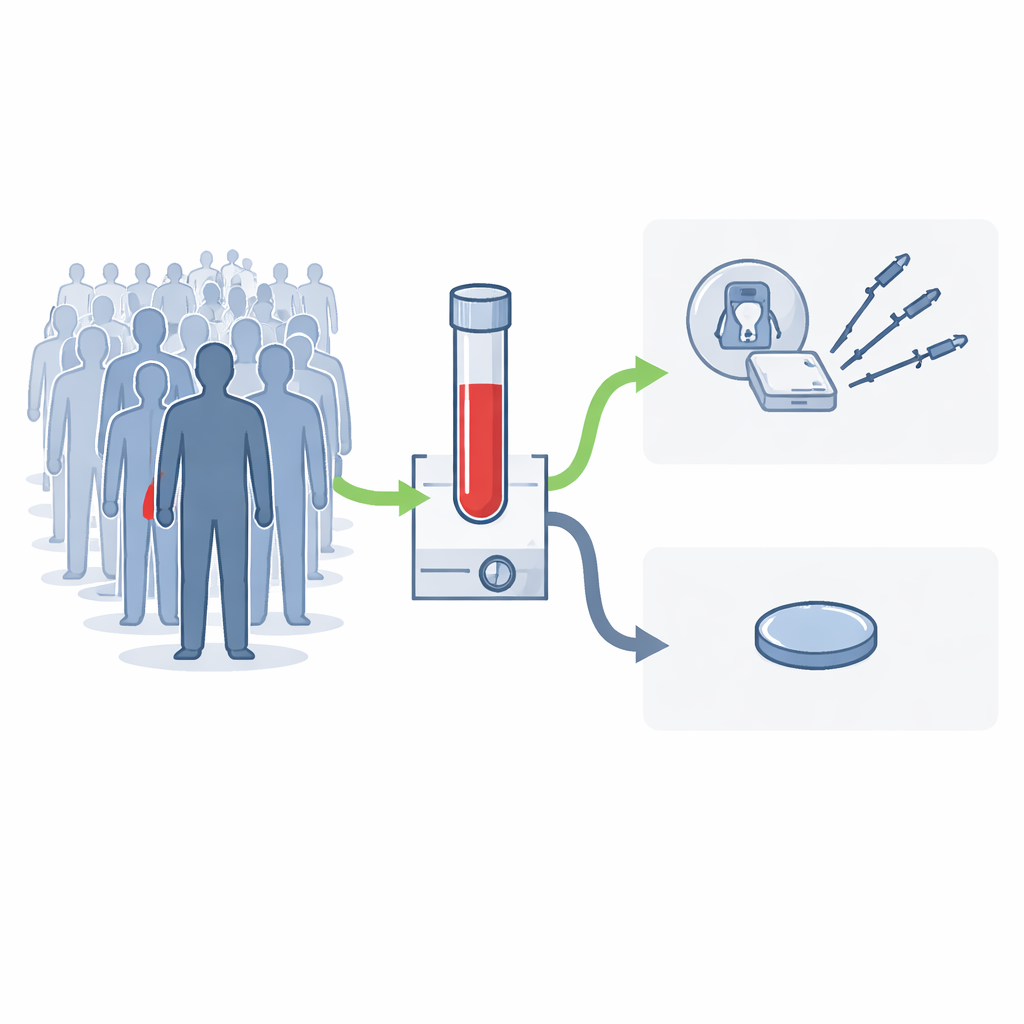
MCED tests look for telltale patterns in tiny fragments of DNA circulating in the blood. If a “cancer-like” pattern is seen, the test reports a cancer signal and suggests where in the body the problem is most likely to be, directing doctors to focus follow-up tests on that area. The team focused on one such test, currently being evaluated in the large NHS-Galleri trial, and modelled what would happen if it were offered every year to everyone in England aged 50 to 79. Their core assumption was that most eligible people would take up the offer, similar to current national screening programmes, meaning around 13 million people screened annually.
Building a realistic picture of test follow-up
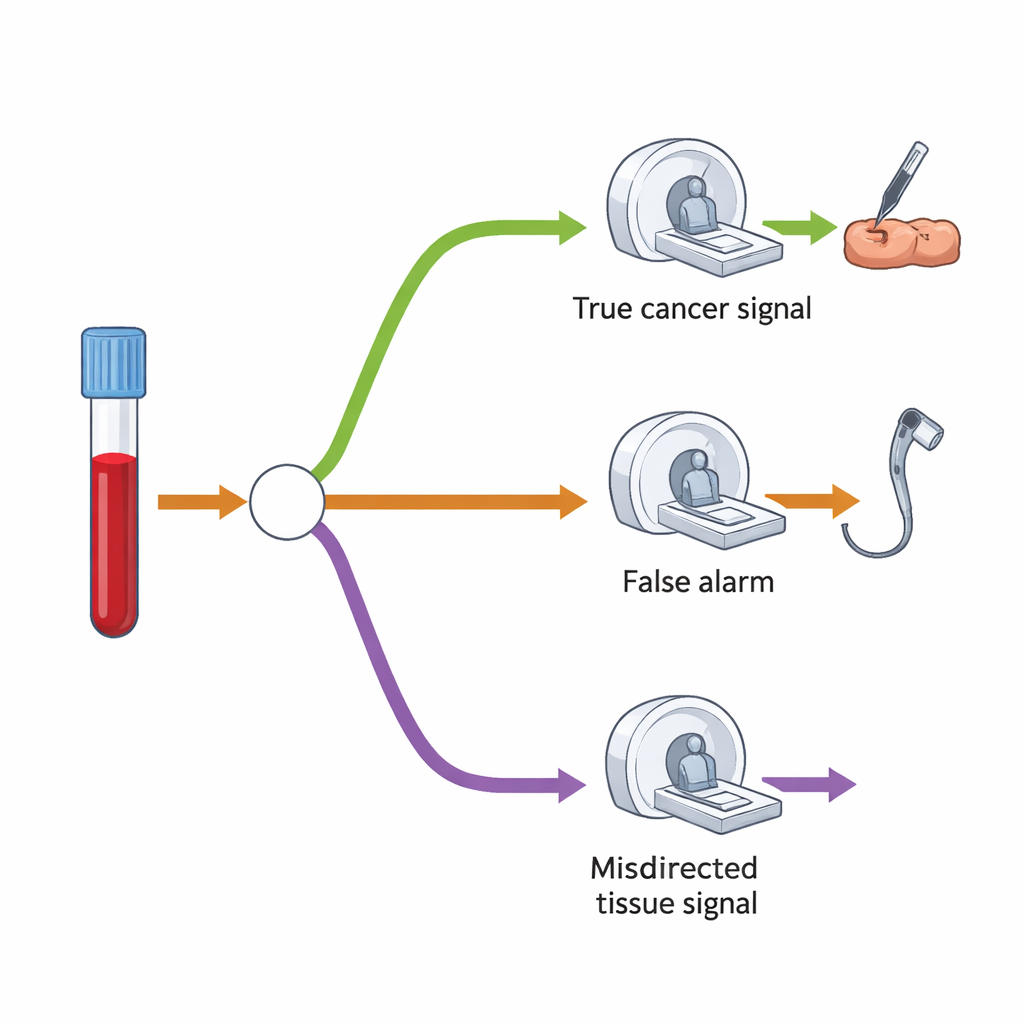
To understand the extra demand on scans and procedures, the researchers built a decision-tree model that maps what typically happens after a “cancer signal detected” result. First, only a small fraction of all those screened are expected to have a positive result—about 1.4%. Among these, some truly have cancer, while others turn out not to. The test is fairly good at guessing the likely organ, but sometimes points to the wrong place. In their model, most people with a positive result would have one main follow-up test—such as a colonoscopy, CT scan, or ultrasound—targeted to the suspected organ. A smaller group, especially when the signal turned out to be wrong or no cancer was found initially, would go on to have a second, more wide-ranging CT scan that examines the chest, abdomen, and pelvis.
How much extra diagnostic work would be needed
The study compared the number of extra tests triggered by MCED screening with how many procedures the NHS already performs each year. In the first years after introducing MCED screening, the biggest relative increases per million people screened would be for colonoscopy and stomach-related endoscopy, followed by biopsies and CT scans. For example, for every million people screened, colonoscopies would rise by about 3,200 procedures in the first round, a 0.49% bump over current yearly activity. CT scans would increase by about 13,200, only a 0.16% rise. When the programme has been running for years and settles into a steady pattern, the impact shrinks further: per million screened, around 1,040 extra colonoscopies and 4,720 extra CT scans—still well under a 1% increase in existing volumes. Even if every single eligible person in England took part, the model suggests that the percentage increases would remain modest compared with the year-on-year growth the NHS already absorbs for many diagnostic services.
Short-term pressure, long-term balance
The authors stress that these modest percentage increases can still mean large absolute numbers of extra procedures, because so many people are eligible for screening. In the short term, this could add to pressure on services such as endoscopy and imaging, which are already stretched. However, the team also notes that MCED screening should shift many cancers from late, symptom-driven diagnosis to earlier, screen-detected diagnosis. Over time, that means fewer people turning up with advanced disease needing urgent tests, which should offset some of the initial surge in demand—especially once the programme reaches a stable rhythm.
What this means for future cancer planning
For patients and the public, the key message is reassuring: adding a broad, blood-based cancer screening test would not swamp the diagnostic system, though it would require careful planning. The model suggests a relatively small increase in demand for scans, scopes, and biopsies relative to what the NHS already delivers each year, with colonoscopy and CT seeing the biggest absolute rises. Because the test may allow many cancers to be caught earlier and more efficiently, the study argues that the extra diagnostic activity is both manageable and potentially worthwhile. Policymakers can use these estimates to plan staff, equipment, and service design so that, if MCED screening is shown to save lives, the health system is ready to support it.
Citation: Martin, J., Jones, D.A., Ellis, L. et al. Modelled impact of a multi-cancer early detection screening programme on the demand for diagnostics in England. Br J Cancer 134, 1190–1197 (2026). https://doi.org/10.1038/s41416-025-03331-8
Keywords: multi-cancer early detection, cancer screening, diagnostic demand, NHS England, CT and endoscopy