Clear Sky Science · en
Intramyometrial injection versus intravenous infusion of oxytocin for maintaining uterine contractility during elective caesarean delivery in a randomised controlled trial
Why this birth medicine study matters
For many families, a planned caesarean birth is a big day that should be as safe and calm as possible. One major concern during any birth is heavy bleeding after the baby is delivered. Doctors routinely use a hormone medicine called oxytocin to help the womb squeeze down and limit blood loss, but this drug can also lower blood pressure and stress the heart. This study explores two different ways of giving oxytocin during planned caesarean delivery, asking which way keeps bleeding under control while keeping a mother’s circulation steady.
Two ways to help the womb contract
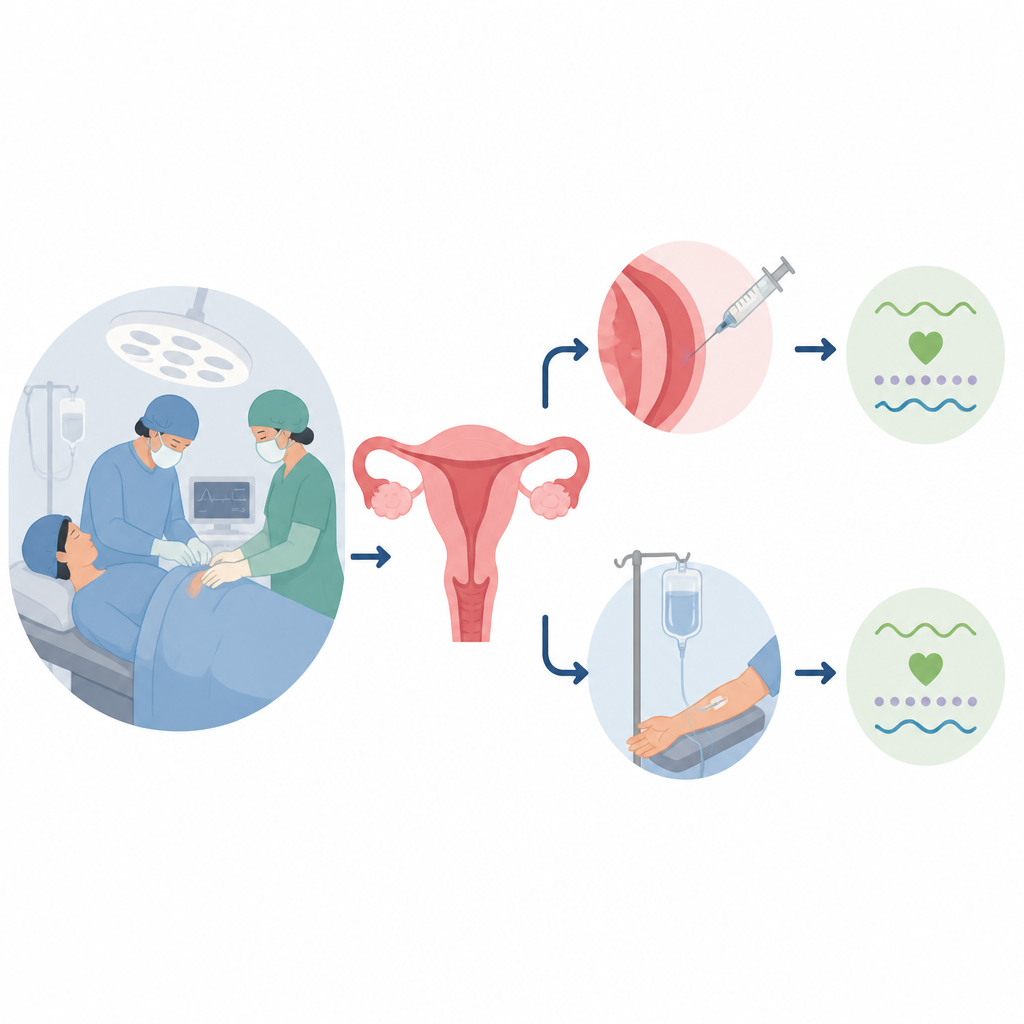
After a baby and placenta are delivered by caesarean section, the womb must clamp down firmly to close off blood vessels. Oxytocin is the standard medicine used worldwide to trigger and maintain these contractions. It can be given through a vein in the arm so it spreads quickly through the bloodstream, or injected directly into the muscle of the womb itself. In Japan, many hospitals choose the direct womb injection, expecting it to work well where it is needed. However, earlier work suggested that, for the first strong squeeze of the womb, vein delivery is more effective. The open question was whether direct womb injection might still be useful for the longer lasting “maintenance” dose that follows the initial push.
How the trial was carried out
The research team in Japan ran a carefully controlled, double blind trial with women having planned caesarean births under spinal or combined spinal epidural anaesthesia. All women first received the same small dose of oxytocin through a vein right after the placenta was delivered. They were then randomly assigned to one of two maintenance plans. In the first, oxytocin was injected into the muscle of the womb, while a harmless saline solution dripped into a vein. In the second, saline was injected into the womb while oxytocin was slowly infused into a vein over two hours. Neither the women nor most of the staff knew which plan was used, and strict rules guided extra medicines if the womb was too soft.
Measuring blood loss and womb firmness
The main question was whether one method led to less blood loss from surgery through two hours after the women returned to the ward. Nurses weighed surgical sponges and measured fluid in suction bottles to carefully estimate total bleeding. Obstetricians also judged how firm the womb felt, and a handheld device pressed on the womb surface provided an objective reading of muscle hardness. The team tracked how often extra oxytocin, other womb tightening drugs, or uterine massage were needed, and noted any serious bleeding that required surgical steps or blood transfusion.
Watching the heart and blood pressure
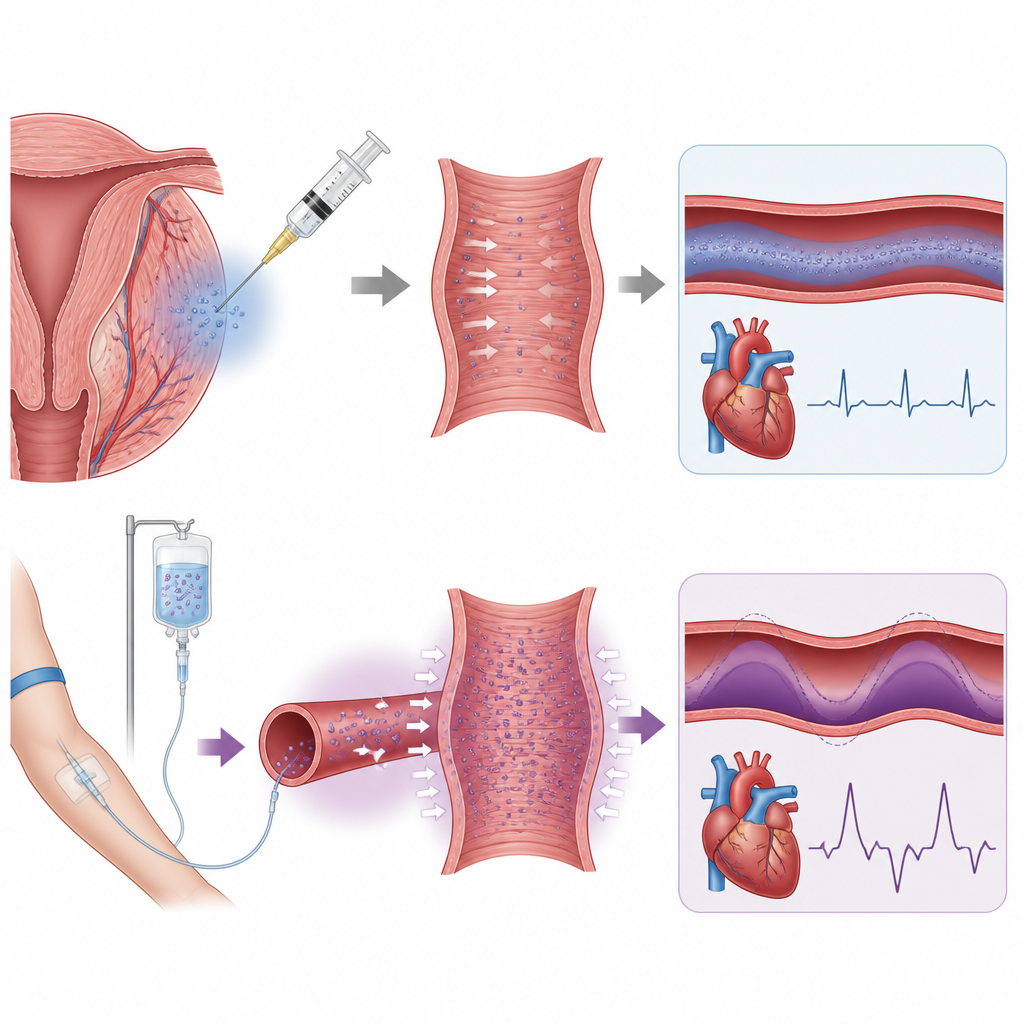
Because oxytocin can suddenly drop blood pressure or speed up the heart, the researchers monitored each woman’s circulation closely. A noninvasive finger cuff system recorded blood pressure, heart rate, and blood flow repeatedly during and after oxytocin administration. If blood pressure fell too low, doctors treated it with another drug called phenylephrine, a standard medicine that tightens blood vessels. The team then compared how much phenylephrine each group needed and how much each woman’s blood pressure drifted from her starting level over the first 30 minutes after oxytocin was started.
What the researchers found
Among the 20 women included in the main analysis, total blood loss was very similar whether the maintenance oxytocin dose was injected into the womb or infused through a vein. The firmness of the womb, as judged by both touch and the hardness meter, also did not differ between the two groups, and the need for extra womb medicines or massage was alike. However, women who received oxytocin directly into the womb had more stable blood pressure and needed less phenylephrine after delivery than those who received the drug by continuous vein infusion. Rates of side effects such as nausea, flushed skin, or shortness of breath were comparable, and no serious complications occurred in either group.
What this means for mothers and doctors
For low risk women having a planned caesarean birth, this small study suggests that directly injecting oxytocin into the womb muscle can control blood loss as effectively as a slow drip into a vein, while causing fewer swings in blood pressure. That added stability could be especially important for women with heart or blood vessel problems, although this trial did not test high risk patients or severe bleeding. The authors stress that in cases of major haemorrhage, usual emergency steps using vein oxytocin and other drugs must still be followed. Larger studies in more diverse women are needed, but the findings offer doctors another evidence based option for balancing safety and comfort in the operating room.
Citation: Naruse, S., Akinaga, C., Mazda, Y. et al. Intramyometrial injection versus intravenous infusion of oxytocin for maintaining uterine contractility during elective caesarean delivery in a randomised controlled trial. Sci Rep 16, 15571 (2026). https://doi.org/10.1038/s41598-026-46727-z
Keywords: caesarean delivery, postpartum haemorrhage, oxytocin, uterine contractility, haemodynamic stability