Clear Sky Science · en
Incidence and risk factors for anastomotic leakage after transanal total mesorectal excision in a retrospective cohort of 212 patients
Why this matters for people with rectal cancer
When surgeons remove a rectal cancer, they often reconnect the bowel so that patients can avoid a permanent stoma bag. The weak point in this operation is the join between the two bowel ends, which can sometimes leak. Such leaks can lead to infections, extra operations, and longer hospital stays. This study looks closely at a modern technique for low rectal cancers, called transanal total mesorectal excision (TaTME), and asks a simple but crucial question: how often does the join leak, and what makes leaks more likely?
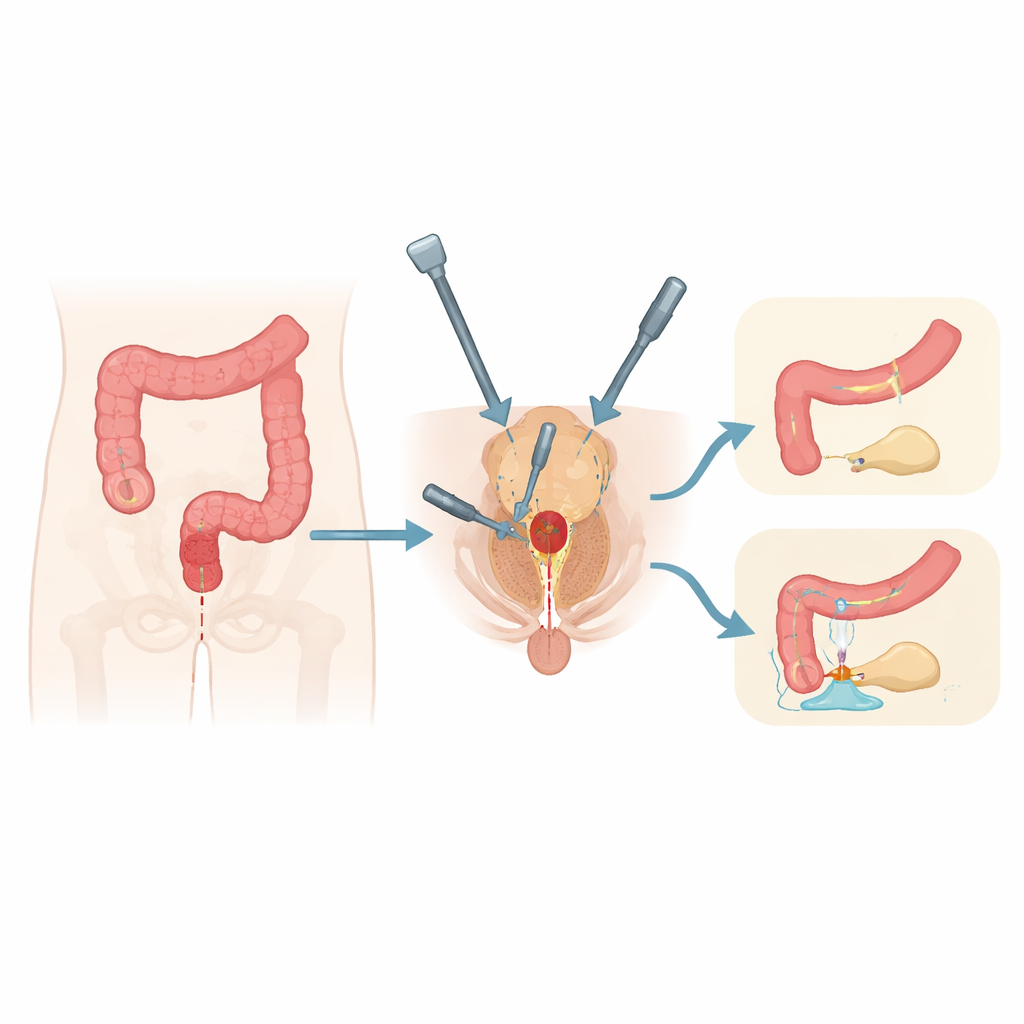
A new way to reach hard-to-operate tumors
Tumors very low in the rectum are hard to reach through the abdomen alone. TaTME tackles this problem by approaching the rectum from two directions at once: from the belly with keyhole instruments and from below through the anal canal. This two-team method can help surgeons see better, work more precisely in the narrow pelvis, and remove the tumor while preserving the anal sphincter. For many patients who might previously have faced a permanent colostomy, TaTME offers a chance to keep natural bowel passage—making the safety of the bowel join especially important.
Who was studied and how
The research team reviewed 237 people with low rectal cancer who underwent TaTME at a single specialist center between 2016 and 2024. In 229 of them, the bowel was reconnected after the tumor was removed. After excluding patients without reliable follow-up, 212 people were analyzed in detail. The investigators collected information on age, sex, general health, body mass index, tumor height above the anal canal, type of join between the bowel ends, pre-treatment with radiation or chemotherapy, use of imaging dye to check blood flow, and whether surgery was done laparoscopically or with a partly open approach. They then tracked how many patients developed a leak at the join and how severe the leak was.
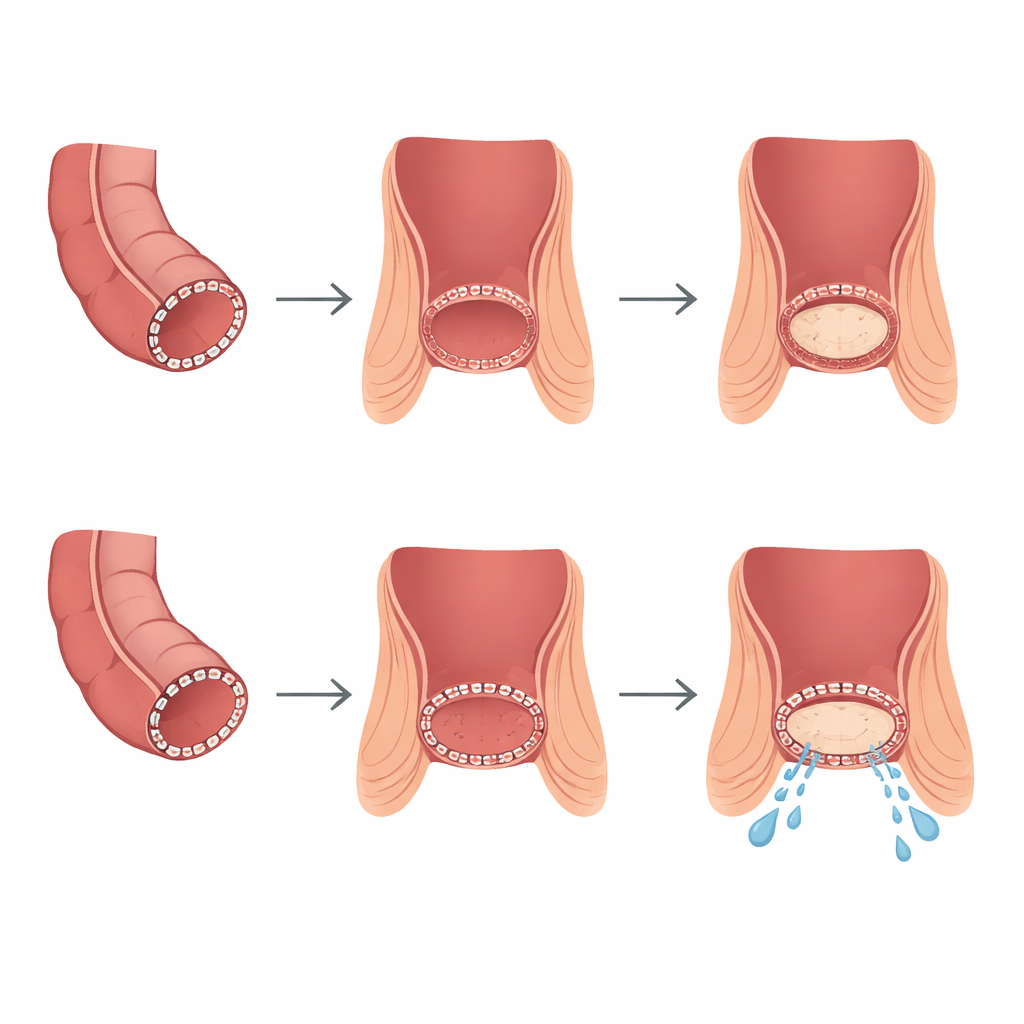
How the join was made
Surgeons used two main ways to reconnect the bowel. When enough rectum below the tumor was available, they favored a circular stapling device that creates a mechanical ring-shaped join. When tumors were extremely low—often within 2 centimeters of the anal sphincter—there was not enough space to use the stapler. In those cases, surgeons hand-sewed the connection directly to the anal canal. Almost all patients received a temporary ileostomy, a small opening on the abdomen diverting stool away from the fresh join to give it time to heal. The team defined leaks according to international criteria, ranging from silent imaging findings to serious problems that required an emergency re-operation.
How often leaks occurred and what raised the risk
Among the 212 patients with reliable data, 27 developed a leak, giving a leakage rate of about 12.7 percent—similar to large international TaTME registries and to other standard rectal cancer operations. Most leaks were mild, but about 5 percent of all patients had more serious leaks that required active treatment or another surgery. When the researchers compared patients with and without leakage, most common risk markers—such as age, overall fitness, weight, prior chemoradiotherapy, type of main surgical access, and use of blood-flow dye—did not clearly change the leak rate. The factor that stood out was how the join was created. Leaks happened in 18.3 percent of patients with a hand-sewn connection but only 8.5 percent of those with a stapled join. Statistical models that considered several variables at once confirmed that, whenever anatomy allowed it, a stapled join was linked with a lower chance of leakage. Tumor height also mattered: the lower the tumor sat in the rectum, the higher the leak risk, and each extra centimeter above the anal junction appeared to cut that risk roughly in half.
What this means for patients and surgeons
The study suggests that TaTME, when done by experienced teams, offers bowel-preserving surgery for very low rectal cancers with leakage rates comparable to other techniques and sound cancer control. For individual patients, the message is that the level of the tumor and the way the bowel ends are joined both play key roles in the safety of the operation. If there is enough room to use a stapler, this method seems to lower the chance of a leak. When tumors are so low that only a hand-sewn connection is possible, the operation becomes more demanding and the risk of leakage rises, even with a protective ileostomy. The authors conclude that TaTME is a feasible option in expert centers but stress that larger, multi-hospital studies are needed to refine how surgeons choose the best joining method and to ensure these results apply more widely.
Citation: Kapturkiewicz, B., Kazanowski, M., Lesiak, P. et al. Incidence and risk factors for anastomotic leakage after transanal total mesorectal excision in a retrospective cohort of 212 patients. Sci Rep 16, 12102 (2026). https://doi.org/10.1038/s41598-026-40735-9
Keywords: rectal cancer surgery, transanal total mesorectal excision, anastomotic leakage, stapled versus hand-sewn anastomosis, low rectal tumors