Clear Sky Science · en
Current status and future perspectives on the mechanistic and pathophysiological understanding of long COVID
Lingering illness after a “mild” infection
For many people, COVID-19 did not end when the acute fever and cough faded. Months later, they still live with crushing fatigue, brain fog, dizziness, breathlessness, or sleep problems—a condition now widely known as Long COVID. This review article pulls together the latest science on what might be causing these long-lasting symptoms, why they vary so much from person to person, and what it will take to diagnose and treat them effectively.
A common problem with many faces
Long COVID is not a rare curiosity. Depending on how it is defined and measured, tens to hundreds of millions of people worldwide have experienced ongoing symptoms after SARS-CoV-2 infection. These problems can appear even after mild or symptom-free cases, and they can affect nearly every organ system, with more than 200 different complaints reported. Many patients are unable to work or manage daily tasks, driving large personal, health-system, and economic costs. Yet there is still no single agreed-upon test, no clear-cut case definition, and no approved cure—only emerging clues and experimental approaches.
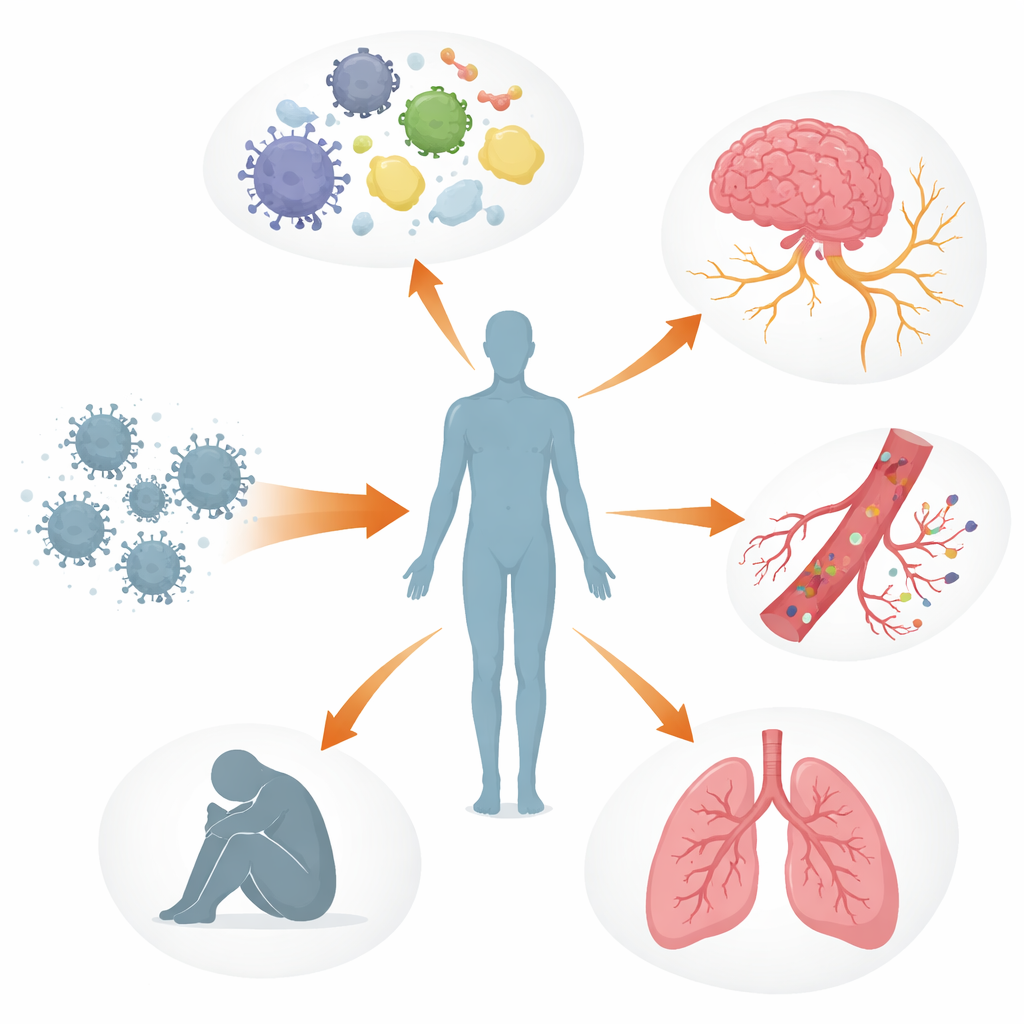
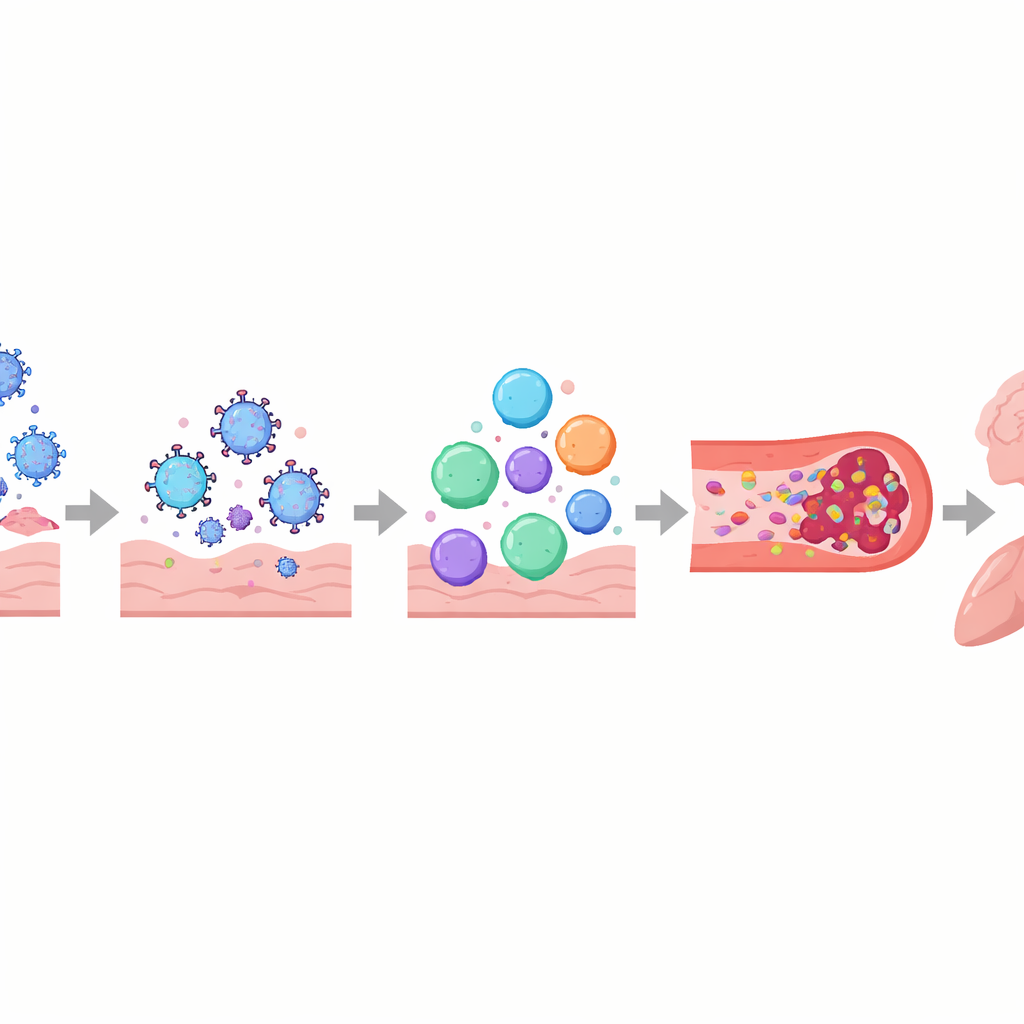
Multiple body systems out of balance
The authors describe Long COVID as a multi-layered disturbance of the body’s control systems rather than damage to one organ alone. The immune system may remain switched on or misdirected, with altered signaling molecules, exhausted virus-fighting cells, and, in some people, antibodies that appear to attack the body’s own tissues, including nerves and blood vessels. In parallel, bits of virus or viral proteins can linger in places like the gut, brain, and lymph nodes for months to years. These hidden reservoirs may keep poking the immune system, contributing to ongoing inflammation and the reawakening of other dormant viruses such as Epstein–Barr virus. Blood vessels and the delicate lining that keeps them healthy can also be injured, encouraging platelets to clump and form tiny, stubborn “microclots” that may restrict oxygen delivery to muscles, brain, and other organs.
How common symptoms may arise
These tangled processes help explain some of the most troubling experiences reported by people with Long COVID. Damage to the automatic nervous system and small nerve fibers, along with low blood volume and microclots, can lead to dizziness and racing heart on standing, often diagnosed as postural orthostatic tachycardia syndrome (POTS). In the brain, leaky blood–brain barriers, viral remnants, and activated immune cells may contribute to brain fog, headaches, and mood changes. In the lungs, persistent inflammation and subtle blood-flow problems can cause air trapping and poor oxygen exchange, even when standard scans look nearly normal. In skeletal muscle, poor blood supply, mitochondrial sluggishness, and structural damage appear to underlie severe fatigue and the phenomenon of post-exertional malaise—where even minor physical or mental effort triggers days or weeks of worsened symptoms.
Living with limits and pacing energy
Because no proven disease-modifying treatments yet exist, symptom management is crucial. The paper argues that one-size-fits-all “just exercise more” advice can be harmful, especially for those who experience post-exertional crashes. Instead, many patients rely on pacing—carefully planning activity to stay within their personal energy limits, often aided by heart-rate or other wearable monitors. Early trials are exploring drugs that dampen misdirected immune responses, clear problematic antibodies, target viral reservoirs, or improve microcirculation, but results are mixed so far and often limited to small, highly selected groups.
What needs to happen next
The authors conclude that Long COVID is best understood as a group of overlapping biological subtypes rather than a single disorder. They call for large, carefully designed studies that combine symptom tracking, imaging, lab tests, and wearable data to sort patients into meaningful categories and identify reliable markers in blood or tissues. Such “precision medicine” approaches could make it possible to match people to targeted therapies instead of trial-and-error care. Until then, Long COVID will continue to strain health systems and economies, and millions will remain disabled by an illness that began with an infection many were told would pass in a couple of weeks.
Citation: Faghy, M.A., Wüst, R.C.I., Altmann, D.M. et al. Current status and future perspectives on the mechanistic and pathophysiological understanding of long COVID. Commun Med 6, 255 (2026). https://doi.org/10.1038/s43856-025-01300-z
Keywords: long COVID, post-viral illness, immune dysregulation, microclots, post-exertional malaise