Clear Sky Science · en
A cadaveric feasibility study of the LM-B screw as a novel posterolateral C1 lateral mass to C2 vertebral body fixation trajectory
A New Way to Stabilize a Fragile Part of the Neck
Injuries high in the neck, just beneath the skull, can be life-changing. This region houses the spinal cord and important blood vessels that feed the brain, so any surgery there is delicate. The study described here explores a new pathway for placing a stabilizing screw between the first and second neck bones in donated human specimens. The goal is to find a route that stays inside the bone while keeping a safe distance from the spinal cord and a critical blood vessel called the vertebral artery. 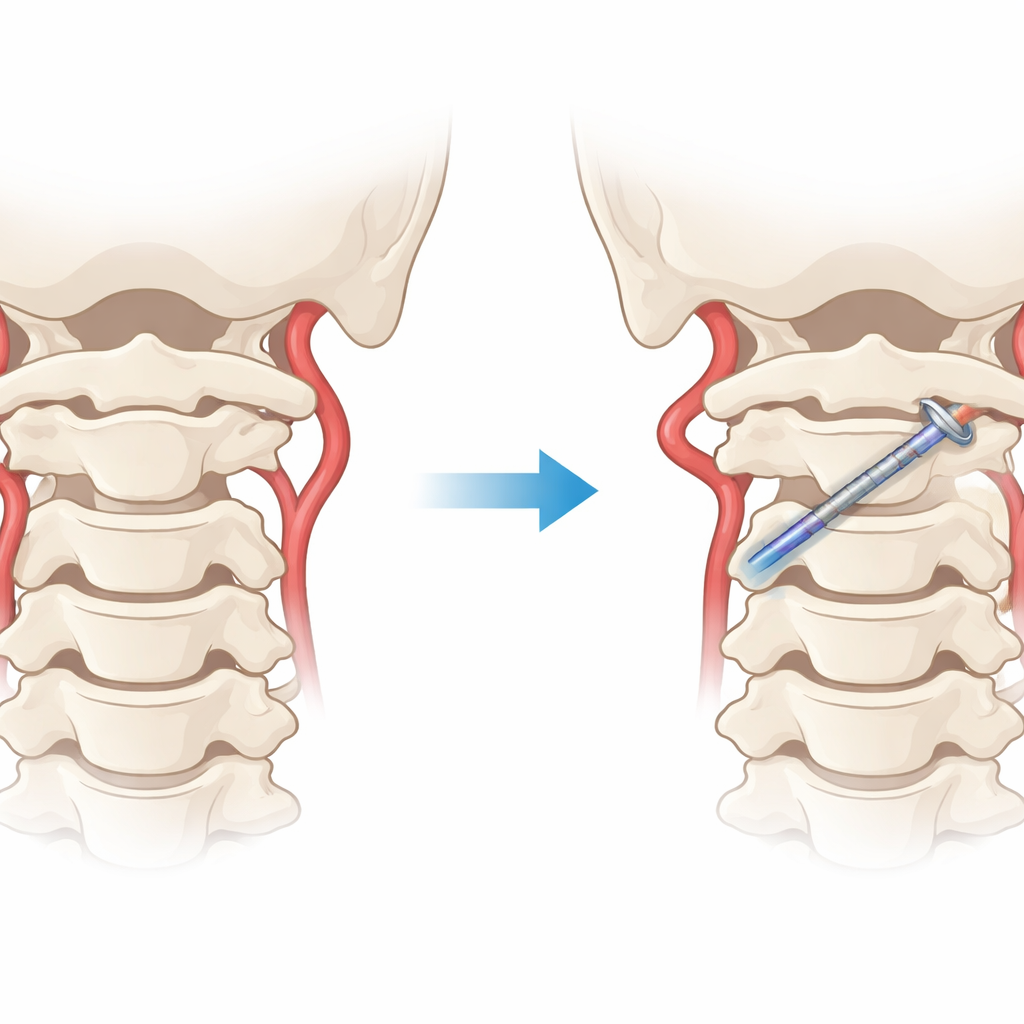
Why This Part of the Neck Is So Hard to Treat
The junction between the first (C1) and second (C2) neck bones is designed for motion: it lets us nod and turn our heads. That same mobility, however, makes it vulnerable to serious injury in high‑energy accidents. When this area is unstable, surgeons often join C1 and C2 using screws and rods so the bones can fuse. Existing techniques work well in many patients but can be risky in people whose bone shape or blood vessel course is unusual. In some, the vertebral artery runs higher or more inward than usual, or the bony bridge that surgeons would normally use for screw placement is too narrow. In these cases, traditional screw pathways may bring the hardware dangerously close to vital structures.
A Different Route for the Screw
The authors propose a new screw path they call the lateral mass–to–body, or LM-B, trajectory. Instead of passing through the usual bony corridor in C2, this screw starts from a consistent spot on the back of C1—where its arch, side block, and side projection meet—and then travels forward and downward into the solid central portion of C2. The idea is to stay entirely within bone while threading a route that skirts above and away from the vertebral artery canal, which houses the artery as it climbs toward the brain. By defining this path precisely, the researchers hope to expand the surgical options when standard routes are blocked by unusual anatomy.
Testing the Pathway in Donated Spines
To see whether this route was even possible, the team worked with four donated human cervical spines preserved in formalin. They placed LM-B screws on both the right and left sides, for a total of eight screws, using live X‑ray imaging to guide the placement. They then scanned the specimens with high‑resolution computed tomography (CT) and built three‑dimensional models. These images allowed them to trace the screw paths slice by slice, check whether the screws ever left the bone, and measure how much they had to angle inward and downward to reach the C2 body. In all specimens, the screws followed a continuous intrabony course, did not enter the spinal canal, and did not break into the bony channel containing the vertebral artery.
What the Measurements Reveal
The CT reconstructions showed that the entry point on C1 could be found reliably in every specimen. The screws typically needed to be angled about one‑third of a right angle both toward the midline and toward the feet to reach their target. The average segment of screw that lay completely within bone was a little under 4 centimeters long. The researchers also mapped out how much the angle could vary before the screw would risk touching either the spinal canal or the artery canal, defining a “safe window” of directions. Although there were minor differences from one side to the other and among specimens, none required changing the basic route, and no cortical breaches or vessel encroachments were seen. 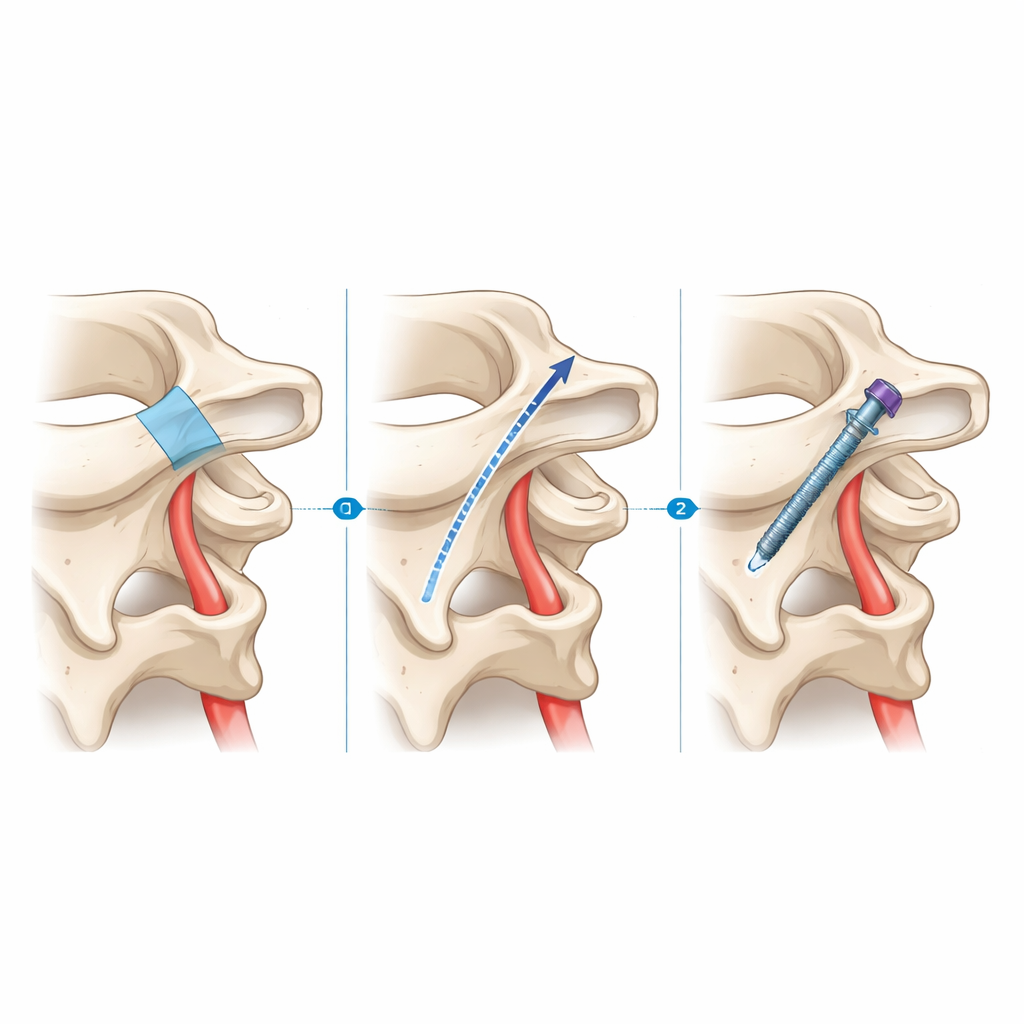
How This Compares and What It Might Mean for Patients
Today’s surgeons already have several ways to fix C1–C2, both from the front and from the back of the neck. Each method carries trade‑offs in strength, complexity, and risk to nearby nerves and vessels. The LM-B route stands out because it offers screw purchase in the sturdy core of C2 while starting from a familiar posterior exposure and steering away from the usual “danger zones” around the vertebral artery and spinal canal. At the same time, the required downward tilt is steep, which could be hard to achieve in patients with a short neck or a prominent skull base, and might demand more extensive dissection than standard techniques.
What This Study Does—and Does Not—Show
For non‑specialists, the key message is that this work does not introduce a new operation ready for the clinic, but rather maps out a promising path through the bony landscape of the upper neck. In this small series of donated spines with typical anatomy, the LM-B screw pathway proved anatomically feasible: it stayed inside bone and clear of the vertebral artery canal in every case. The study does not yet tell us how strong this construct would be, how it performs under real‑world loads, or whether it is safer or better than existing options. Future studies will need to test its mechanical strength and evaluate it in live patients, especially those whose anatomy makes current methods difficult. If those hurdles are cleared, this new pathway could someday give surgeons another tool to stabilize one of the most delicate junctions in the human body.
Citation: Topal, B., Güvenç, Y. A cadaveric feasibility study of the LM-B screw as a novel posterolateral C1 lateral mass to C2 vertebral body fixation trajectory. Sci Rep 16, 10601 (2026). https://doi.org/10.1038/s41598-026-45865-8
Keywords: atlantoaxial fusion, vertebral artery, cervical spine surgery, screw fixation, craniovertebral junction