Clear Sky Science · en
Clinical feasibility of intratracheal tracheostomy sealing using a novel sealing disc prototype
Helping patients breathe and speak after a neck tube
When people spend weeks on a breathing machine, doctors sometimes create a small opening in the neck, called a tracheostomy, to place a tube into the windpipe. Removing that tube is a major step toward recovery, but the leftover hole can leak air, weaken the cough, and make it hard to speak clearly. This study tests a small silicone disc that seals the opening from the inside of the windpipe, with the aim of making breathing, coughing, and healing easier during the days after the tube is removed. 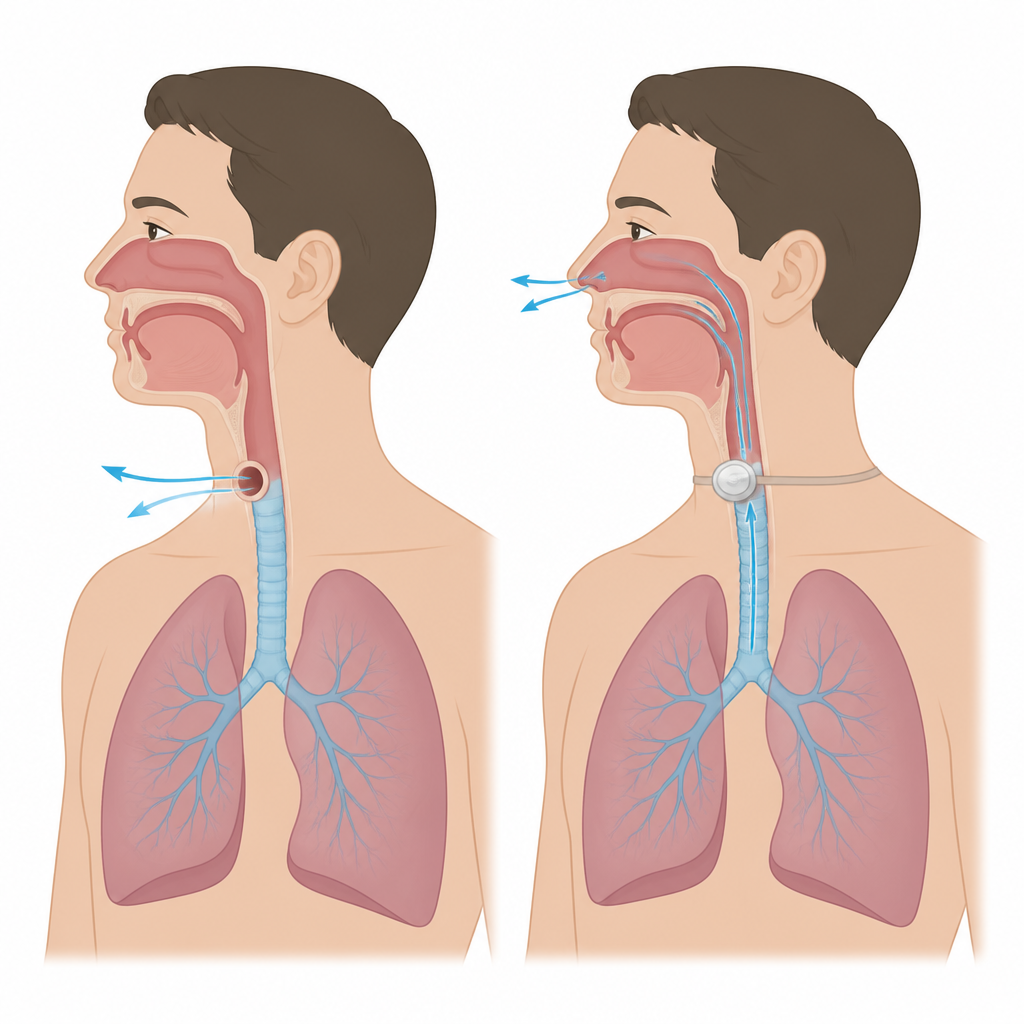
The problem with an open throat opening
After the tracheostomy tube comes out, the neck opening usually closes on its own over one to two weeks. Until then, every breath and every cough can leak through that hole instead of flowing normally through the mouth and nose. This leakage can weaken the cough, trap mucus in the lungs, and interfere with common breathing therapies that rely on steady pressure. It can also make speech quiet and breathy because not enough air passes the vocal cords. Standard dressings and gauze placed over the skin are often not airtight, can be messy to maintain, and may slow down healing.
A small disc placed inside the windpipe
The team behind this study developed a thin silicone disc that sits just inside the windpipe and plugs the tracheostomy from within. The disc is attached to a narrow silicone “tail” that passes out through the opening and connects to a soft neck band on the skin. To insert it, clinicians fold the disc into a special tube, slide it through the tracheostomy channel, and then let it spring open against the inside wall of the windpipe. To remove it, they gently pull the tail so the disc curls into a slim strip and slips out through the healing opening with little resistance. Safety features, including a small thickened area where the disc meets the tail and an external bridge, help keep the device from slipping out accidentally during coughing or movement. 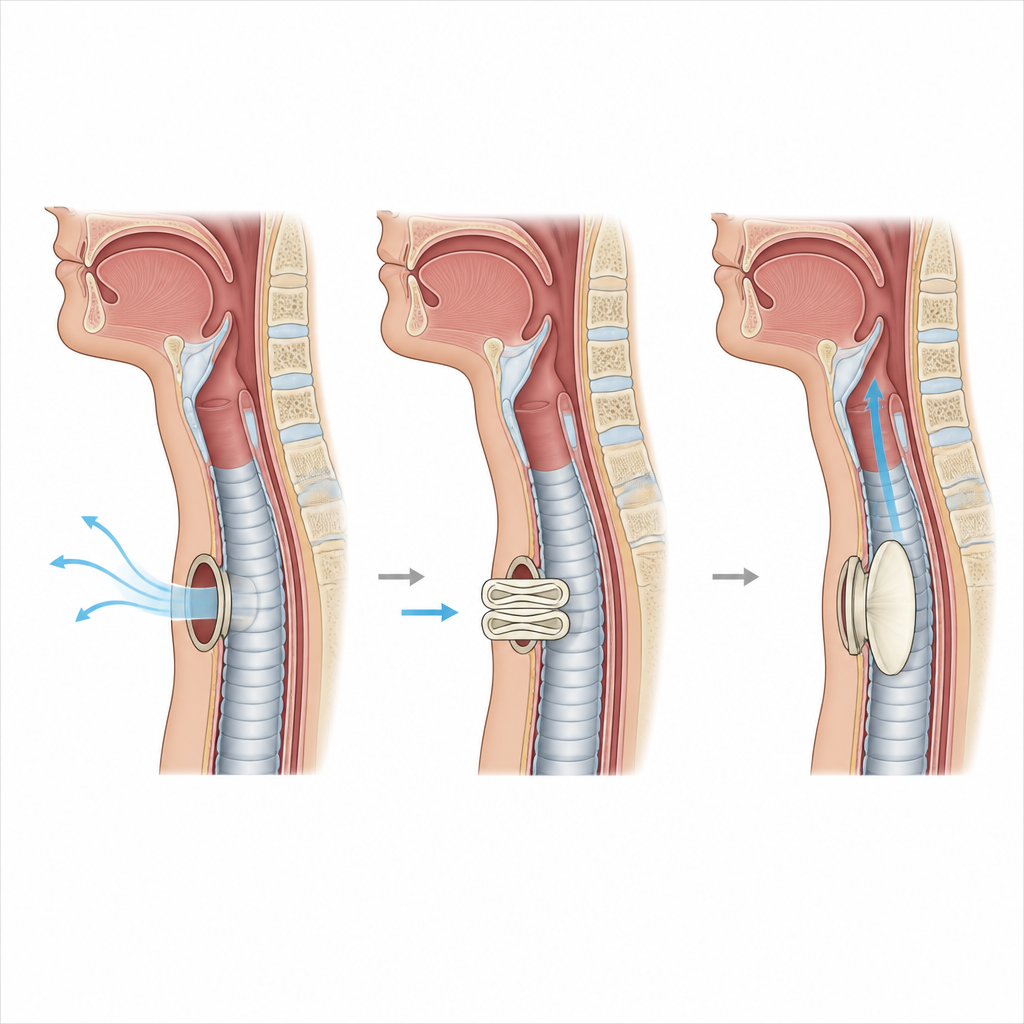
How the study was carried out with patients
The researchers first ran a pilot phase in eleven patients to fine tune how the disc was placed and secured. Early problems with slight air leakage and discomfort were solved by adjusting the insertion tube, placing the disc a bit deeper at first, and shortening the time between tube removal and disc insertion. They then conducted a main study in ten adults in intensive care who had been on a ventilator and had their tracheostomy for more than a week. Immediately after the breathing tube was removed, doctors measured lung function and voice with the neck opening left uncovered, then inserted the disc and repeated the tests. These checks were repeated daily until the skin had tightened around the tail of the device, usually by day three or four, when the disc was removed and lung and voice tests were repeated once more.
What happened to breathing, voice, and healing
In all ten main-study patients, the disc was placed and removed quickly and without device problems. Patients did not report discomfort once the final insertion method was used, and all were able to cough out mucus without needing suction through the windpipe. Measurements of lung function showed that key values such as the amount of air the lungs could blow out and how fast it could be expelled rose right after the disc was put in and stayed stable while it was worn. Voice recordings improved from nearly inaudible just after tube removal to near normal while the disc was in place, and this better voice quality largely remained even after the disc came out. Most patients said it was easy to speak and to clear mucus, and overall satisfaction scores on a simple five point scale were at the top end.
How the neck wound closed
The skin around the tail of the disc tightened in three to four days for all patients, at which point the device was removed. The remaining opening was only a few millimeters wide, and in most of the patients who could be checked again one to two days later, the hole in the airway had closed completely and no air leaked out. This suggests that holding the inner opening firmly shut may not only protect breathing while the device is in place but also help the tissue close faster afterward. One patient did need to return to intensive care and be reintubated after the disc was removed, because mucus built up when a small opening remained, highlighting that some patients may still need close monitoring even with improved sealing.
What this could mean for future care
For patients coming off long term ventilation, the days after tracheostomy tube removal are a fragile period. This first in human study suggests that a simple silicone disc inside the windpipe can safely seal the neck opening, improve breathing tests and voice, and support quick, clean wound healing, all while being well accepted by patients. The work is early and involved only a small group without a comparison group using standard dressings, so larger controlled trials are needed. If future studies confirm these findings, intratracheal sealing discs could become a new tool to make decannulation safer, reduce the need for repeat ventilation, and allow patients to breathe, cough, and talk more naturally during recovery.
Citation: Kraghede, R.E., Nielsen, L.W., Christiansen, K.J. et al. Clinical feasibility of intratracheal tracheostomy sealing using a novel sealing disc prototype. Sci Rep 16, 14800 (2026). https://doi.org/10.1038/s41598-026-41209-8
Keywords: tracheostomy, decannulation, airway sealing, lung function, voice recovery