Clear Sky Science · en
Comparison of ventilation with second-generation supraglottic airway devices in a prospective randomized cadaver study
Why breathing tools matter in emergencies
When someone needs help breathing during surgery or after a sudden collapse, doctors must quickly choose the right tool to keep air flowing to the lungs. The standard approach uses a tube placed directly into the windpipe, but this can be slow and technically demanding. Newer devices that sit above the voice box offer a simpler alternative. This study explores how a newly redesigned breathing device performs compared with well known options, using donated human bodies to test how well each tool actually moves air.
Simple devices for a critical job
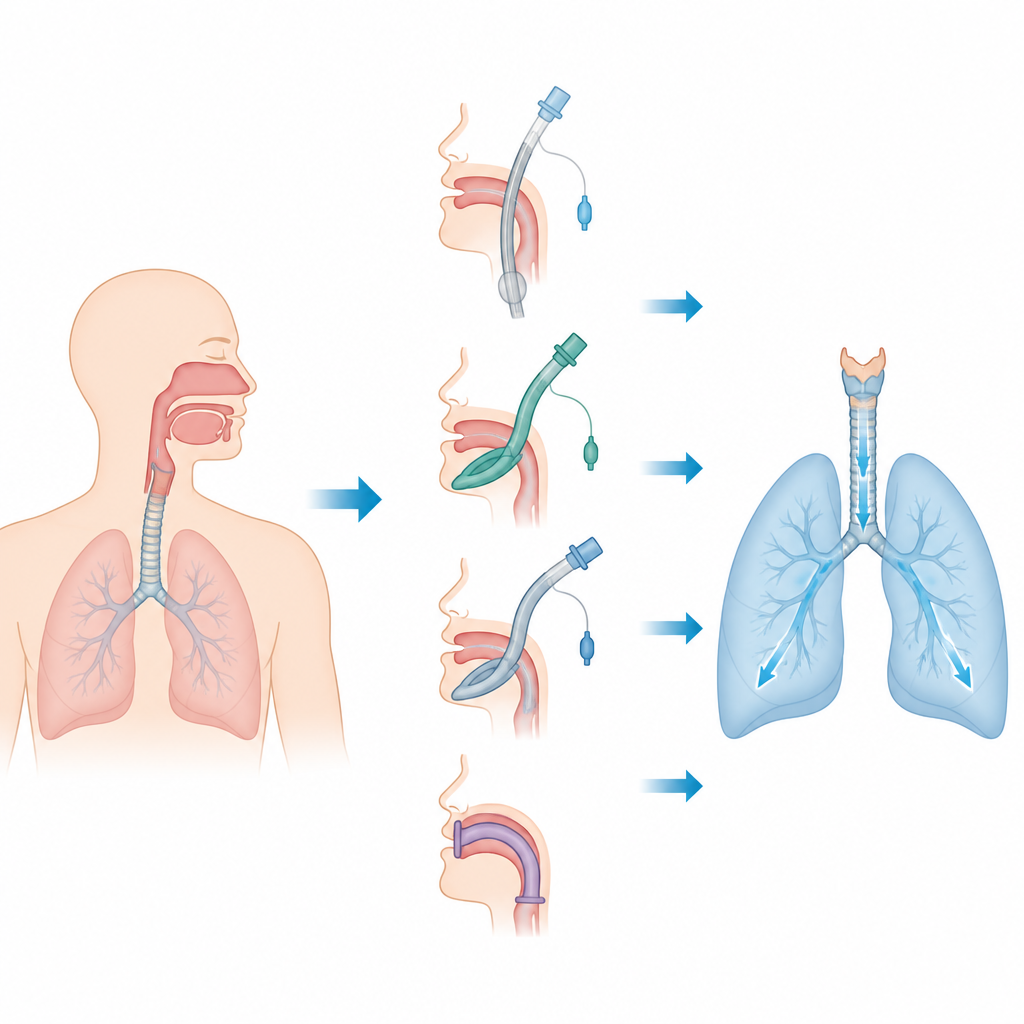
Modern supraglottic airway devices are placed in the mouth and sit just above the entrance to the windpipe. They are widely used in operating rooms and in ambulances when time is short or placing a tube into the windpipe is difficult. The LT®evo is a new version of an older device called the LTS-D. It keeps the same basic idea but reshapes the inflatable sections, widens the air channel, and adds features to keep the flap of tissue called the epiglottis from blocking airflow. Importantly, it is also designed so doctors can later pass a regular breathing tube through it using a tiny camera, turning a quick rescue airway into a more secure one.
Testing breathing support on donated bodies
To compare devices in a controlled way, the researchers used six thawed, non-embalmed adult cadavers. Each cadaver was first given a standard breathing tube to set a reference point. Then, four different supraglottic airway devices plus the standard tube were placed in random order. A ventilator delivered a set volume of air with the same pressure settings each time, while high speed sensors recorded how much air actually reached the lungs and how much pressure and flow were needed. The key measure was the inspiratory tidal volume, which is the amount of air pushed into the lungs with each breath, with a target range based on estimated body weight.
How the new device stacked up
Across 30 complete ventilation runs, the LT®evo delivered almost the same amount of air per breath as the standard endotracheal tube, the older LTS-D, and another popular device called Ambu AuraGain. All of these met the preset threshold for adequate ventilation in this model. By contrast, the i-gel Plus, a soft, cuffless device, moved clearly less air on average and did not reach the adequacy threshold under the test conditions. The standard breathing tube required the highest pressures and resistance, meaning the ventilator had to work harder to push air through it, while the supraglottic devices generally allowed similar or lower pressures. The researchers also confirmed that, once placed correctly, the LT®evo, AuraGain, and i-gel Plus all allowed a breathing tube to be threaded through them using fiberoptic guidance.
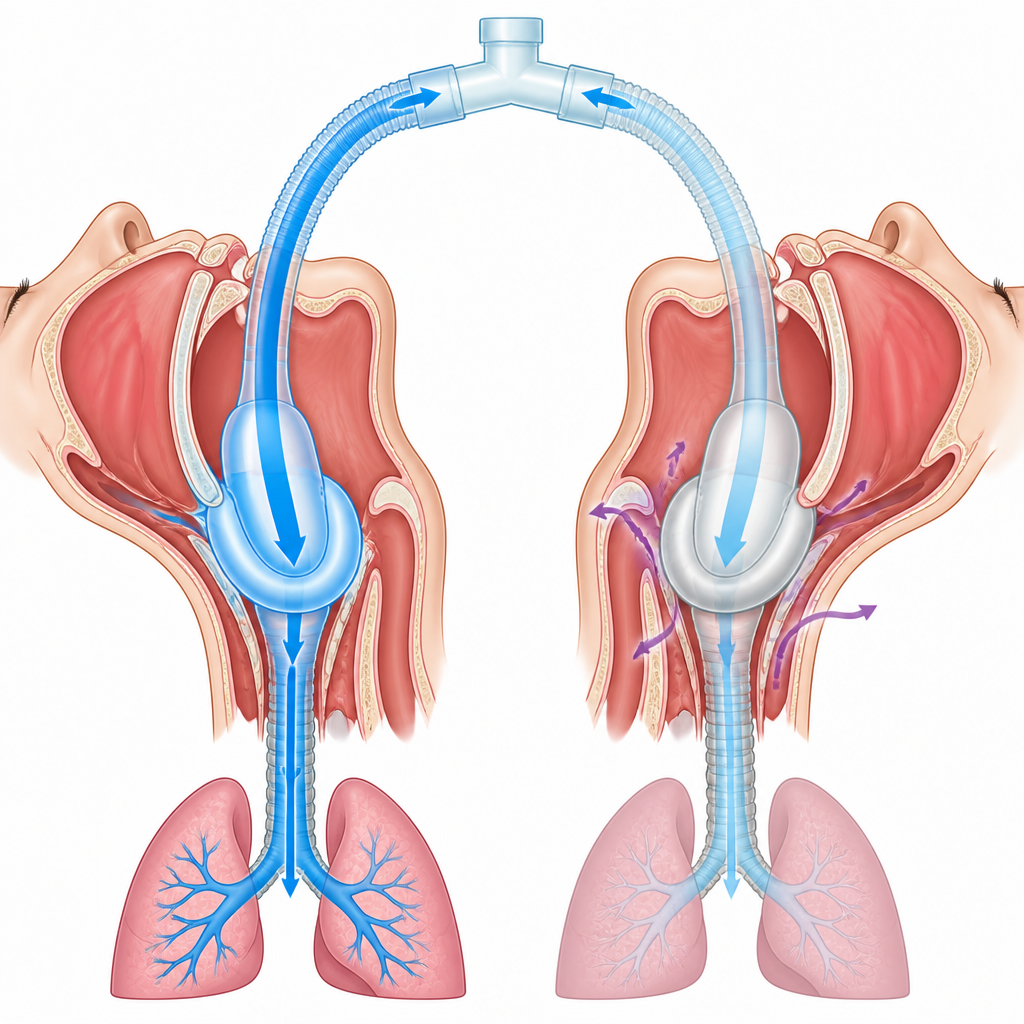
Understanding leaks and fit
The team examined detailed loops that relate pressure and flow to see how each device behaved during breathing cycles. The i-gel Plus showed patterns that matched its lower delivered volumes, suggesting more leakage or a less secure seal in this cadaver setting. Further checks limited to the cadavers with the most consistent measurements showed that, when the seal was good, the i-gel Plus could in fact deliver air volumes similar to the other devices. This points to subtle differences in how well each device conforms to the airway and maintains its seal, rather than a simple yes or no answer about whether they work. The authors stress that the lack of muscle tone, altered tissue stiffness, and cooler temperatures in cadavers may particularly disadvantage devices that rely on body warmth to mold to the throat.
What this means for patient care
Because these tests were done on cadavers, the results speak to mechanical performance rather than real world outcomes such as oxygen levels, comfort, or risk of stomach contents entering the lungs. Still, the study suggests that the new LT®evo can move air as effectively as established devices while adding the useful option of serving as a stable bridge to a standard breathing tube. The apparent shortfall of the i-gel Plus in this model may reflect the special conditions of post-mortem tissue rather than how it behaves in living patients. The authors conclude that larger clinical trials in real patients are needed to see how these differences in air delivery, seal behavior, and pressures translate into everyday anesthesia and emergency care, where speed, safety, and reliability all matter.
Citation: Weilbacher, F., Kaltschmidt, N., Klein, M. et al. Comparison of ventilation with second-generation supraglottic airway devices in a prospective randomized cadaver study. Sci Rep 16, 15873 (2026). https://doi.org/10.1038/s41598-026-53005-5
Keywords: airway management, supraglottic airway, mechanical ventilation, emergency medicine, endotracheal intubation