Clear Sky Science · en
Enhancing aerosol delivery in asthma and COPD: a comparison of MDI, valved holding chamber, and DPI systems using functional respiratory imaging (FRI)
Why this matters for people with breathing problems
For millions of people living with asthma or chronic obstructive pulmonary disease (COPD), relief often comes from a small handheld inhaler. But how much of the medicine in each puff actually reaches the lungs, and how much simply crashes into the back of the throat and is wasted? This study uses advanced medical imaging and computer modeling to compare common inhaler types and shows that pairing a pressurized inhaler with a simple add‑on device called a valved holding chamber can deliver medicine to the lungs more reliably and with fewer unwanted side effects.
Different tools for getting medicine into the lungs
Today, two main types of inhalers are prescribed for obstructive lung diseases. Pressurized metered‑dose inhalers (MDIs) release a fine spray of medicine when the user presses down on the canister, while dry powder inhalers (DPIs) release a cloud of powder when the user inhales sharply. Each design has trade‑offs. MDIs work well but demand good timing between pressing and breathing in; DPIs avoid that timing challenge but often require a fast, forceful breath, which not every patient can manage. A third option, the valved holding chamber (often called a spacer), attaches to an MDI. It acts as a temporary reservoir that slows the spray, filters out large droplets, and lets patients breathe in at their own pace. 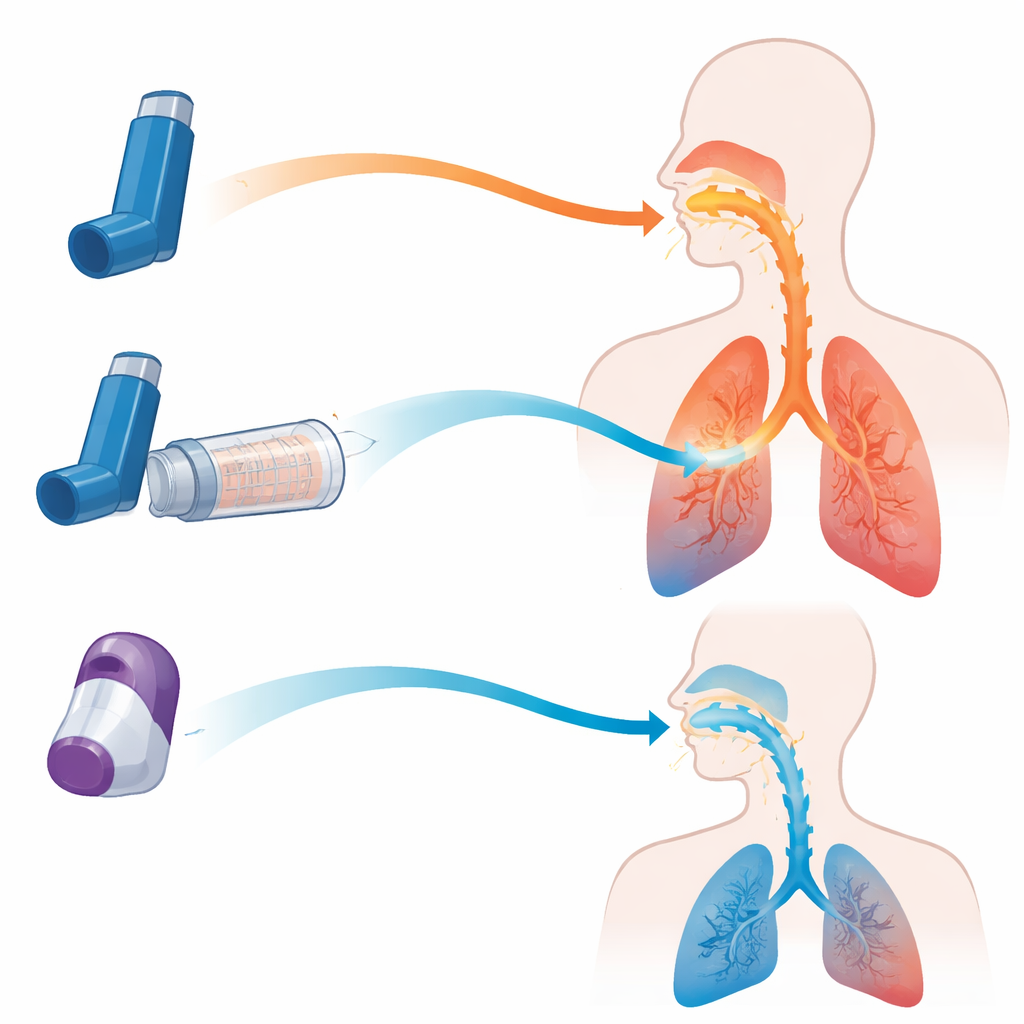
Seeing where the medicine really goes
Instead of relying on simple lab tests or single overall lung measurements, the researchers used a technique called functional respiratory imaging. They combined high‑resolution CT scans of real patients with detailed computer simulations of airflow and tiny particles moving through branching airways. Models were built for one person with COPD and one with moderate asthma. The team then fed in measured particle size data for several devices: an MDI used alone, the same MDI attached to three different holding chambers, and several widely used DPIs. They simulated both ideal breathing patterns and more realistic, less‑than‑perfect inhalation maneuvers to see how much medicine ended up in the throat versus deep inside the lungs.
Timing mistakes can waste almost an entire dose
The simulations revealed just how unforgiving an MDI can be when used without a spacer. When the spray was inhaled at exactly the right moment, roughly one quarter of the dose reached the lungs in the COPD model. But adding a delay of only half a second between pressing the canister and breathing in caused lung delivery to collapse to almost zero, while most of the dose slammed into the mouth and throat. By contrast, when the same MDI was used with a specific holding chamber, lung delivery stayed high even with a two‑second delay, and medicine hitting the throat dropped from about 60 percent of the dose to under 10 percent. In other words, the chamber largely removed the need for perfect coordination and sharply cut the amount of drug that never makes it past the upper airways.
Not all chambers or powder inhalers behave the same
When the study compared three different holding chamber designs, one model consistently delivered nearly twice as much drug to the lungs as the others in both the asthma and COPD simulations, approaching the performance of a perfectly used MDI. This suggests that details such as internal shape, valve behavior, and surface properties can strongly influence how much medicine remains available to be breathed in. The team also compared the best MDI‑plus‑chamber setup with several popular dry powder inhalers under both strong and weaker inhalation efforts. The MDI‑chamber combination delivered more medicine to the lungs and far less to the throat than the powder devices, and its performance hardly changed when the breathing pattern was less than ideal. The DPIs, by contrast, were highly sensitive to flow: they did reasonably well when the simulated breath was strong and fast, but their lung delivery dropped and throat deposition remained high when the inhalation was weaker. 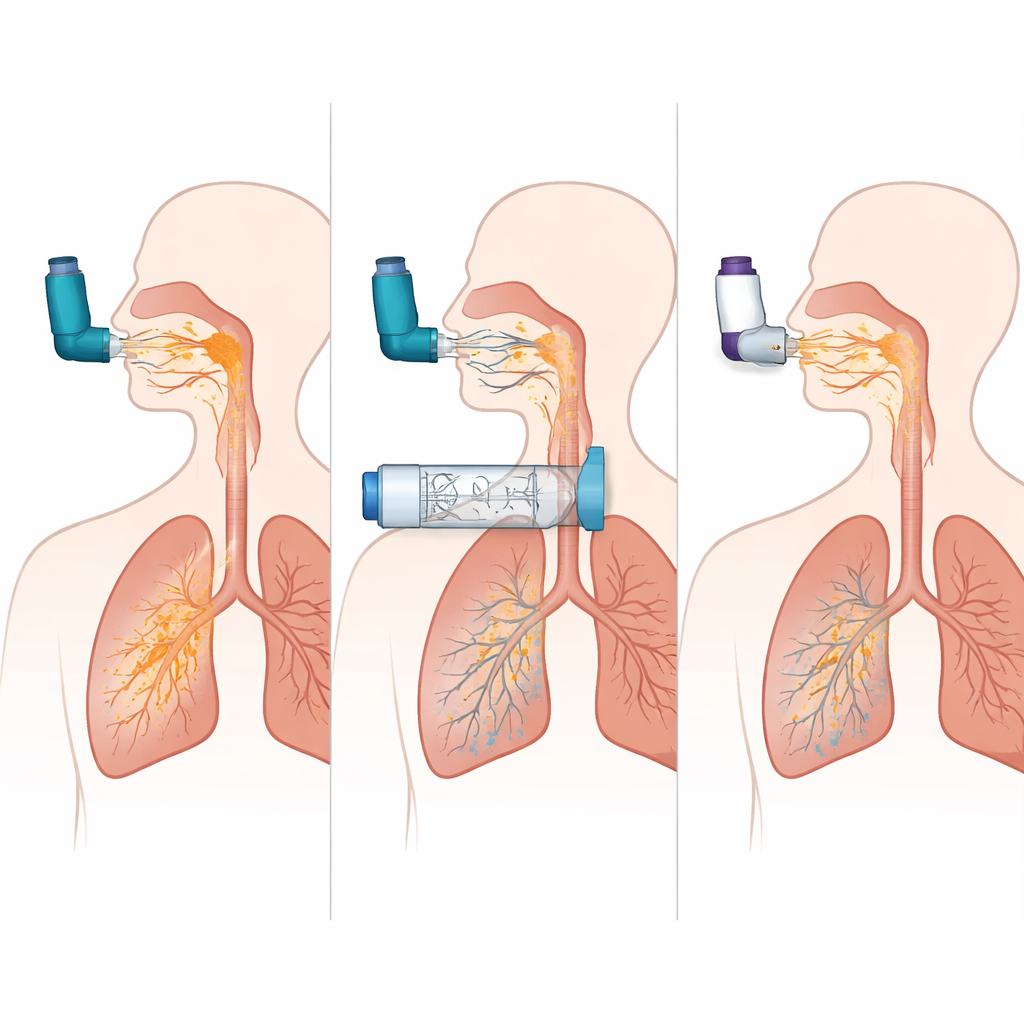
What this means for everyday treatment
Taken together, these findings support a simple, patient‑friendly message. For people with asthma or COPD, especially children, older adults, and anyone who struggles to coordinate their inhaler or take a strong breath, using an MDI with a well‑designed valved holding chamber can make drug delivery both more efficient and more consistent. It sends more medicine where it is needed most—the lungs—while limiting the amount that coats the mouth and throat, where it can cause problems like hoarseness or oral infections. While the study relies on computer models built from a small number of patients and idealized breathing patterns, it suggests that adding the right spacer to an existing inhaler may be one of the simplest ways to improve real‑world control of obstructive lung disease.
Citation: Nagel, M.W., Sadafi, H. & Suggett, J.A. Enhancing aerosol delivery in asthma and COPD: a comparison of MDI, valved holding chamber, and DPI systems using functional respiratory imaging (FRI). Sci Rep 16, 13148 (2026). https://doi.org/10.1038/s41598-026-45628-5
Keywords: asthma inhalers, COPD treatment, spacer devices, dry powder inhaler, aerosol drug delivery