Clear Sky Science · en
Effects of a Pringle maneuver on jejunal mucosal oxygenation and blood flow in a porcine model
Why Surgeons Temporarily Clamp Blood Flow
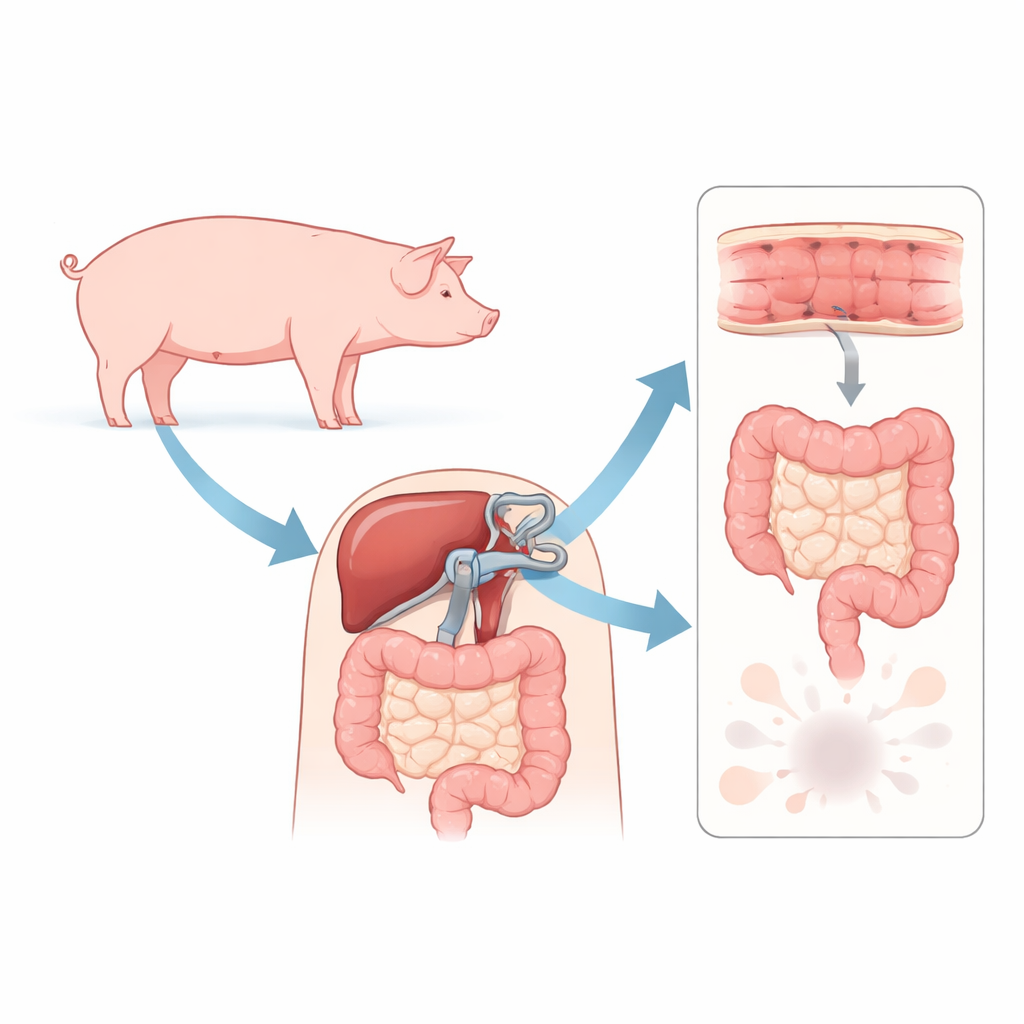
During liver surgery, doctors often pinch off the main vessels that bring blood to the liver to limit bleeding. This move, called the Pringle maneuver, can be lifesaving in the operating room—but it also briefly backs up blood in the intestines. This study in pigs asks a deceptively simple question: when surgeons clamp these vessels for 20–40 minutes, what really happens to oxygen delivery in the delicate inner lining of the small intestine, and could that hidden damage matter for patients later on?
How Blocking Blood Flow Protects and Threatens
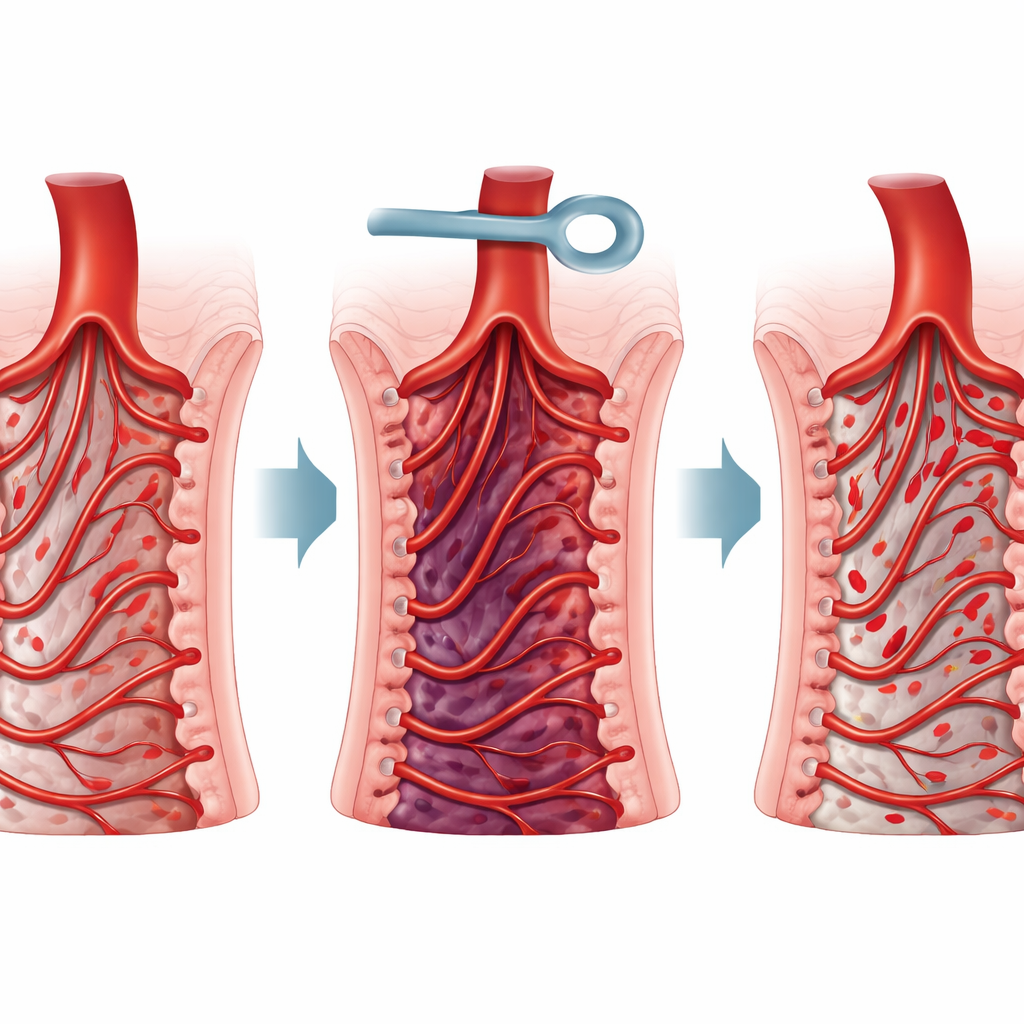
The Pringle maneuver works by tightening a loop around the bundle of vessels entering the liver, sharply reducing blood loss while surgeons cut through liver tissue. Yet that same bundle also carries blood from the gut back toward the liver. When it is clamped, blood can pool in the intestines, creating a form of congestion followed by a surge of flow when the clamp is released. Earlier animal work suggested that the fragile gut lining is especially sensitive both to low flow and to the burst of blood and waste products that return when circulation restarts. The current study focuses on this junction between helpful blood-loss control and potential hidden injury to the gut.
What the Researchers Did in Pigs
Twenty‑three anesthetized pigs underwent a controlled surgical setup that allowed the team to measure blood pressure, heart function, blood flow in the main gut vessels, and fine-scale flow and oxygen levels directly on a small exposed patch of the jejunum, a part of the small intestine. The animals were divided into three groups: one had a 20‑minute clamp, another a 40‑minute clamp, and a control group had no clamping at all. Sensors placed on the bowel surface tracked both how much blood was moving through tiny vessels and how much oxygen actually made it into the mucosa—the thin inner layer that forms the barrier between the gut contents and the rest of the body. Measurements were taken before clamping, during the maneuver, and repeatedly for more than an hour after blood flow was restored.
Blood Flow Recovers, Oxygen Does Not
As expected, clamping the vessels led to a sharp fall in blood flow through the mesenteric artery and portal vein, and to changes in overall circulation such as drops in blood pressure and rises in blood lactate, a marker of stress and poor oxygen use. When the clamp was released, the large-vessel blood flow to the intestines returned to near normal in both clamped groups, and the tiny vessels in the jejunum also showed substantial recovery of flow. However, the oxygen story was very different. The direct readings of oxygen tension and hemoglobin oxygen saturation in the mucosa stayed markedly depressed compared to the control animals, even after flow had come back. This mismatch between restored circulation and persistently low oxygen was stronger and longer‑lasting in the pigs that had been clamped for 40 minutes, which also showed more pronounced and sustained acidosis and lactate elevation.
Why Reperfusion Can Hurt More Than the Blockage
The findings point to reperfusion injury—the damage that occurs when blood rushes back into previously congested tissue—as a major culprit. In this scenario, the returning blood does not distribute evenly through the microvessels; some areas become over‑perfused while others are bypassed, creating “shunting” and patchy oxygen delivery. Inflammatory reactions and changes in the tiny vessels themselves can further interfere with effective oxygen use. The study’s key message is that, for the jejunal mucosa, simply restoring bulk blood flow is not enough. After even 20 minutes of clamping, and more clearly after 40 minutes, the gut lining remains functionally under‑oxygenated despite apparently adequate flow in the larger vessels.
What This Means for Patients and Future Surgery
For a general reader, the bottom line is that a blood‑saving technique in liver surgery may quietly strain the small intestine’s protective lining, especially when the clamp is kept on for longer stretches. The work suggests that the harm is driven less by the period of reduced flow itself and more by what happens when flow returns. Because the intestinal mucosa helps keep bacteria and toxins inside the gut, a lasting oxygen shortfall could weaken this barrier and promote wider inflammation in the body. While the study was done in healthy pigs and cannot be directly translated to humans with illness, it reinforces the idea that clamping times should be kept as short as practical and that strategies to soften reperfusion injury may be as important as controlling bleeding in the first place.
Citation: Sartori, S., Pajk, W., Kleinsasser, A. et al. Effects of a Pringle maneuver on jejunal mucosal oxygenation and blood flow in a porcine model. Sci Rep 16, 12622 (2026). https://doi.org/10.1038/s41598-026-42933-x
Keywords: liver surgery, intestinal oxygenation, reperfusion injury, Pringle maneuver, gut barrier