Clear Sky Science · en
Intraoperative fluorescence-guided fresh frozen sectioning for margin control in head and neck cancer: phase 2 clinical trial
Sharper Cancer Surgery While You Sleep
For people facing surgery for cancers of the mouth, one of the biggest worries is whether the surgeon can remove all of the tumor in a single operation. If cancer cells are left too close to the cut edge, patients may need more surgery, radiation, or chemotherapy, each bringing its own risks and side effects. This study tests a new way to help surgeons and pathologists see, during the operation itself, exactly how close they are cutting to the cancer, so they can adjust on the spot instead of days or weeks later.
Why Clean Edges Matter
In head and neck cancer surgery, doctors aim to remove the tumor with at least a 5-millimetre “safety belt” of healthy tissue around it. When that belt is too thin, patients are more likely to see the cancer return and more likely to need extra treatment afterward. Today, pathologists often check only small samples of the removed tissue while the patient is still in the operating room. This frozen-section technique is specific but can miss dangerous spots simply because it cannot sample every edge. As a result, many patients still wake up with margins that are too close, and surgeons may later have to go back into an area that has already started to heal or has been rebuilt.
Lighting Up Hidden Cancer
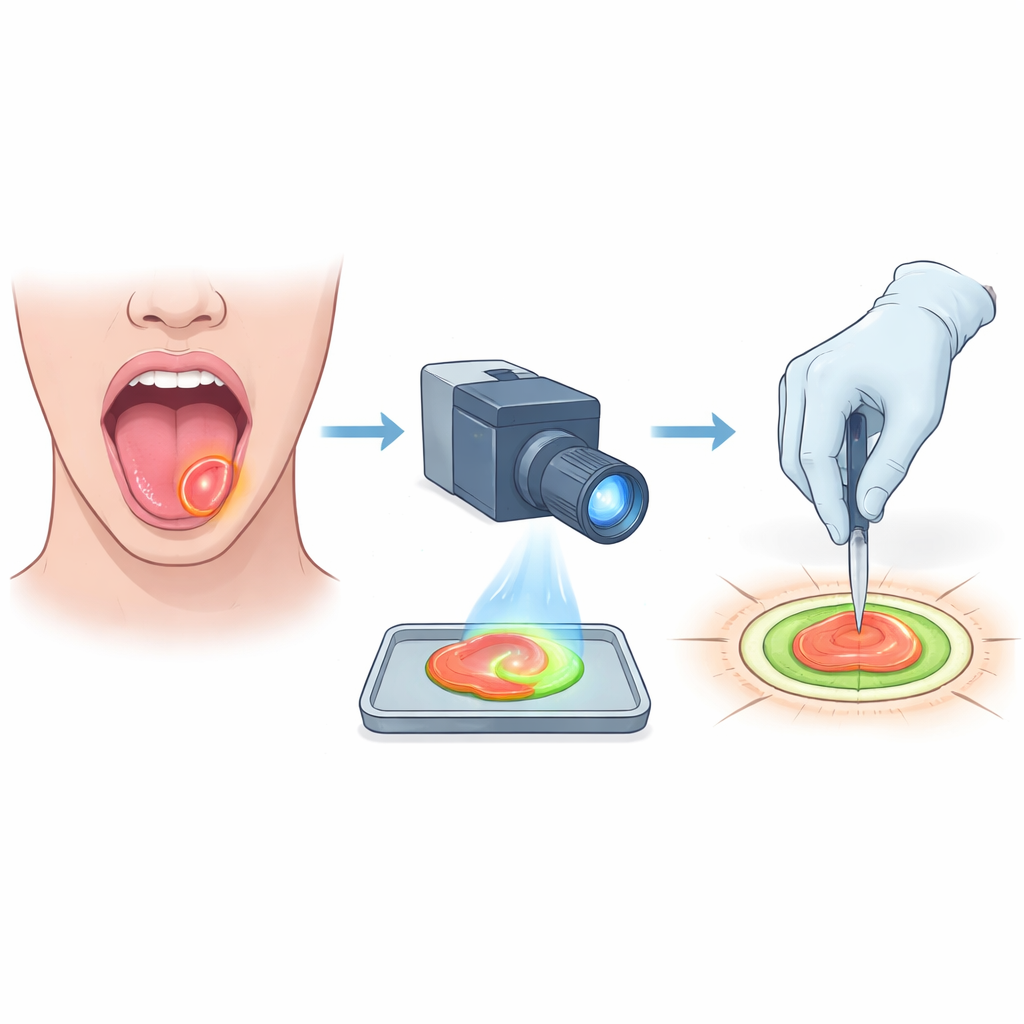
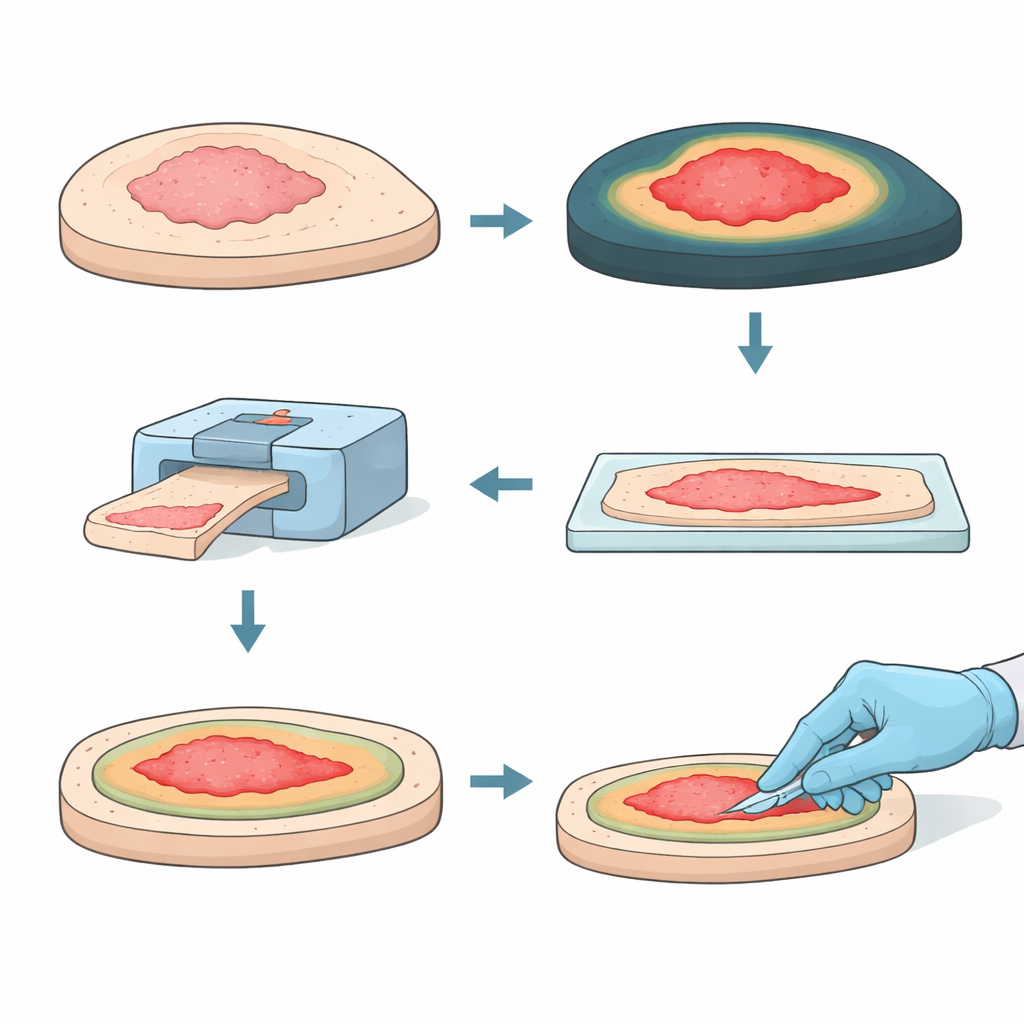
The researchers tried a different strategy that combines a glowing drug with rapid microscopic analysis. Two days before surgery, patients received a special antibody attached to a near-infrared dye. This antibody seeks out a protein that is abundant on oral cancer cells, causing tumor areas to glow when viewed with a dedicated camera. After the surgeon removed the tumor, the entire specimen was sliced into thin slabs and imaged for fluorescence. Bright regions suggested places where the cancer came close to the cut surface. Those suspect spots were then examined under the microscope using a frozen-section slice, giving an exact measurement of how many millimetres of healthy tissue lay between tumor and edge.
Testing the Approach in Real Operations
In this phase 2 clinical trial, 20 patients with cancers of the mouth, mostly of the tongue, underwent surgery with this combined fluorescence-guided, fresh frozen sectioning approach. Without the new method, standard surgery would have left half of these patients with margins considered inadequate. Using the glowing tracer to steer where pathologists took their frozen sections, the team correctly classified margin status in 19 of the 20 patients while the operation was still underway. When the new method showed that cancer was too close to the edge, surgeons could immediately remove a bit more tissue from the matching spot in the mouth, guided by small paired tags that linked each part of the specimen back to its original location.
Fewer Close Calls, Less Extra Treatment
This real-time guidance had a striking impact. Eight of the nine patients identified in the operating room as having risky margins had immediate extra tissue removed. In seven of them, this second, targeted cut turned their status from unsafe to safely clear when full lab analysis was done later. Overall, the share of patients with inadequate margins fell from 50% to 15%. For many, that meant avoiding or scaling back follow-up radiation or chemoradiation: seven of the ten patients who would otherwise have needed margin-based extra treatment were able to skip it or receive a milder regimen. Importantly, all of this extra checking and re-cutting fit within about an hour of operating time and did not delay the surgeries.
What This Means for Patients
To a person on the operating table, the main question is simple: did they get it all this time? This study shows that using a tumor-seeking glow plus targeted quick-look microscopy can give surgeons a much clearer answer while the patient is still asleep. By more accurately spotting and fixing tight spots around the tumor in real time, the method sharply reduces the chance of leftover cancer at the edge and lowers the need for harsh extra treatments afterward. Although the fluorescent drug can cause allergic reactions in a few patients and the technique still needs testing in larger, randomised trials, it offers a promising route toward safer, more precise cancer surgery with better odds of a single, successful operation.
Citation: Nijboer, T.S., Keizers, B., Boeve, K. et al. Intraoperative fluorescence-guided fresh frozen sectioning for margin control in head and neck cancer: phase 2 clinical trial. Nat Commun 17, 3769 (2026). https://doi.org/10.1038/s41467-026-70264-y
Keywords: oral cancer surgery, surgical margins, fluorescence-guided surgery, frozen section pathology, head and neck oncology