Clear Sky Science · en
Esophageal cancer: from pathogenesis to precision therapies
Why this cancer matters to you
Esophageal cancer affects the tube that carries food from the mouth to the stomach, and it is among the deadliest digestive cancers worldwide. Because early disease often causes few or no symptoms, many people are diagnosed only when swallowing is already difficult and treatment options are limited. This review pulls together what scientists now know about how esophageal cancer starts, how it grows, and how doctors are learning to detect it earlier and treat it in more personalized ways that could eventually improve survival.
Two main cancer types, many different risks
Esophageal cancer actually comes in two major forms. One, called squamous-cell carcinoma, tends to arise in the middle and upper part of the esophagus and is especially common in parts of Asia and Africa. It is strongly linked to smoking, heavy alcohol use, very hot drinks, certain food preservatives, and poor nutrition. The other, adenocarcinoma, usually appears where the esophagus meets the stomach and is more common in Western countries. It is associated with chronic acid reflux, a condition called Barrett’s esophagus in which the lining changes its character, and with obesity and smoking. Together these cancers caused almost half a million deaths worldwide in 2022, and men are affected far more often than women.
From healthy lining to tumor
Both cancer types develop through a stepwise journey rather than appearing overnight. In squamous-cell carcinoma, years of irritation from tobacco, alcohol, or other exposures can push the flat surface cells of the esophagus through stages of thickening, abnormal growth, and finally invasive cancer. In adenocarcinoma, repeated acid and bile reflux can transform the normal lining into Barrett’s tissue, which can then progress through low-grade and high-grade precancerous changes before turning malignant. Along this path, cells accumulate DNA damage, lose key safeguards such as the TP53 “guardian” gene, and pick up extra copies of growth-promoting genes. The authors describe how modern “multi-omics” tools, which read DNA, RNA, proteins, and chemical tags on the genome, are revealing detailed maps of these changes and helping to distinguish lesions that are likely to stay stable from those that are primed to become cancerous. 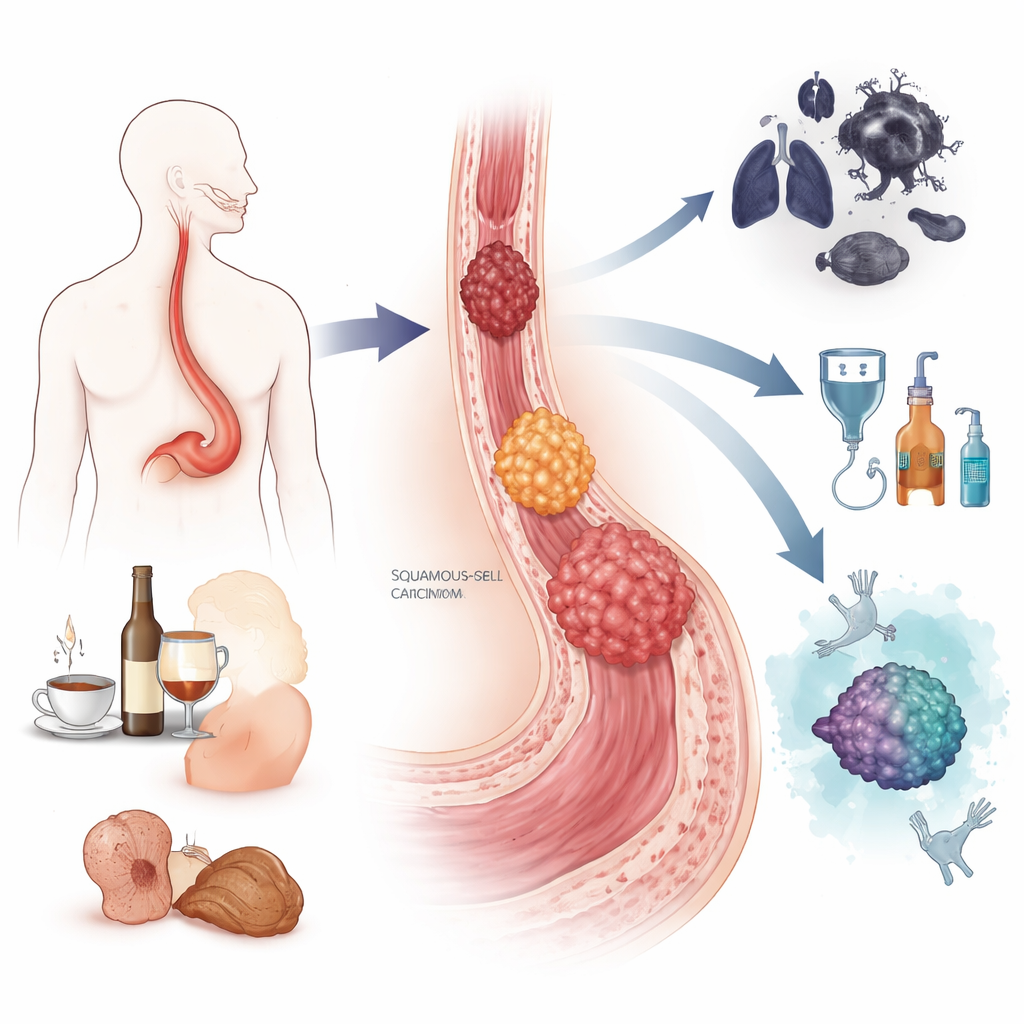
The neighborhood around the tumor
Cancer cells do not evolve alone: they constantly communicate with their surroundings. In the esophagus, pre-cancerous and cancerous cells interact with supporting cells called fibroblasts, immune cells that can either attack or protect tumors, blood vessels, and even resident bacteria. Over time, normal fibroblasts are “educated” into cancer-associated fibroblasts that help remodel tissue, build a protective scaffold around the tumor, and shield it from chemotherapy and immune attack. Early on, immune cells can recognize and destroy abnormal cells, but as the tumor advances, it often creates a more suppressive environment filled with exhausted T cells and specialized macrophages that dampen anti-cumor responses. Shifts in the local microbiome, such as overgrowth of certain mouth bacteria, may further fan chronic inflammation or even blunt responses to treatment.
Prevention, early detection, and less invasive treatment
Because so many risk factors are related to lifestyle and environment, prevention has real power. Quitting smoking and limiting alcohol use can greatly reduce the risk of squamous-cell cancer over time, while weight control, managing acid reflux, and healthy diets rich in fruits and vegetables may cut the risk of adenocarcinoma. In regions with very high rates, large-scale endoscopy programs have shown that looking directly at the esophageal lining and removing precancerous lesions can lower deaths. New tools aim to make screening more comfortable and affordable: swallowable sponges that collect cells, blood tests that detect cancer-specific DNA methylation patterns, saliva microRNA profiles, and artificial-intelligence systems that help endoscopists spot tiny lesions. When caught early, many esophageal cancers can now be removed through endoscopic techniques or treated with targeted ablation, sparing patients major surgery and offering cure rates above 90 percent. 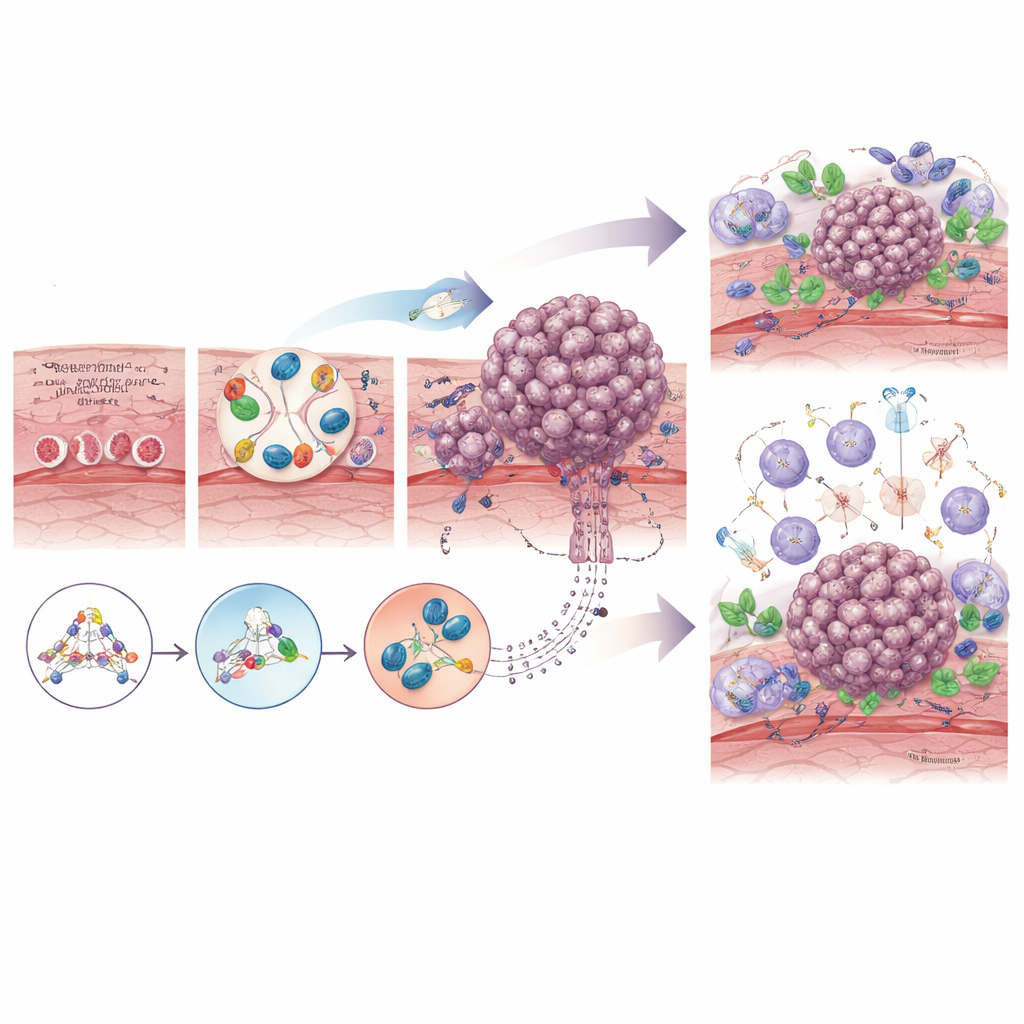
Toward precision therapies for advanced disease
For more advanced tumors, the standard backbone remains surgery, chemotherapy, and radiation, but treatment is becoming increasingly tailored. Some adenocarcinomas overproduce specific receptors such as HER2 or VEGFR2, which can be blocked by targeted drugs added to chemotherapy. In both major subtypes, immune checkpoint inhibitors—drugs that release the brakes on T cells—have improved survival when combined with chemotherapy or given after chemoradiation and surgery. Researchers are also testing combinations of immunotherapy with radiation or targeted agents, and exploring next-generation approaches such as CAR-T and TCR-engineered T cells. At the same time, they are using genetic and immune signatures to predict who is most likely to benefit and to understand why others relapse, with the goal of overcoming resistance.
What this means for patients and the future
The review concludes that esophageal cancer, once viewed as a uniformly grim diagnosis, is entering an era of more precise prevention and care. By clarifying how everyday exposures, inherited tendencies, and microenvironmental changes cooperate to drive tumors, scientists are beginning to identify people at highest risk long before symptoms appear and to design screening tools suited to different settings. For those who do develop cancer, detailed molecular profiling is guiding choices among endoscopic therapy, surgery, chemotherapy, targeted drugs, and immunotherapy. Much work remains to make early detection widely accessible and to tackle treatment resistance, but the emerging picture is one of steady progress—moving from one-size-fits-all approaches toward interventions that are better timed, less invasive, and more closely matched to each person’s tumor biology.
Citation: Zhang, S., Shen, Y., Zhu, L. et al. Esophageal cancer: from pathogenesis to precision therapies. Sig Transduct Target Ther 11, 134 (2026). https://doi.org/10.1038/s41392-026-02614-7
Keywords: esophageal cancer, Barrett’s esophagus, cancer screening, tumor microenvironment, immunotherapy