Clear Sky Science · en
One-year outcomes of an innovative laparoscopic pectopexy procedure using inverted T-mesh for treatment of advanced uterine and anterior vaginal prolapse
Why this matters to everyday women
Many women, especially after childbirth or with aging, experience a distressing problem called pelvic organ prolapse, where the uterus or vaginal walls sag downward. This can cause pressure, discomfort, bladder problems, and pain during sex, yet many suffer in silence. This study explores a new minimally invasive keyhole operation that aims to lift and support both the uterus and the front vaginal wall at the same time, with the hope of faster recovery, preserved sexual function, and fewer bowel problems than existing operations.
A new way to lift and support
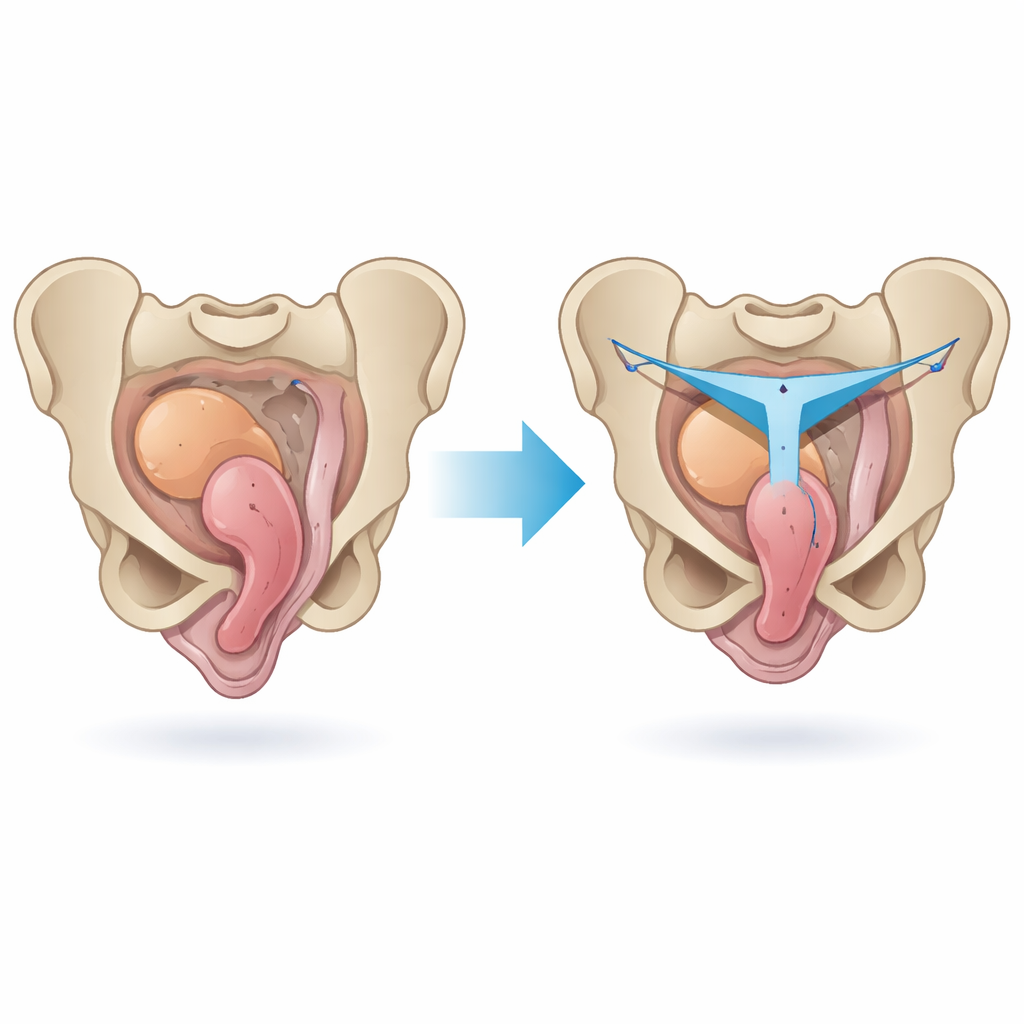
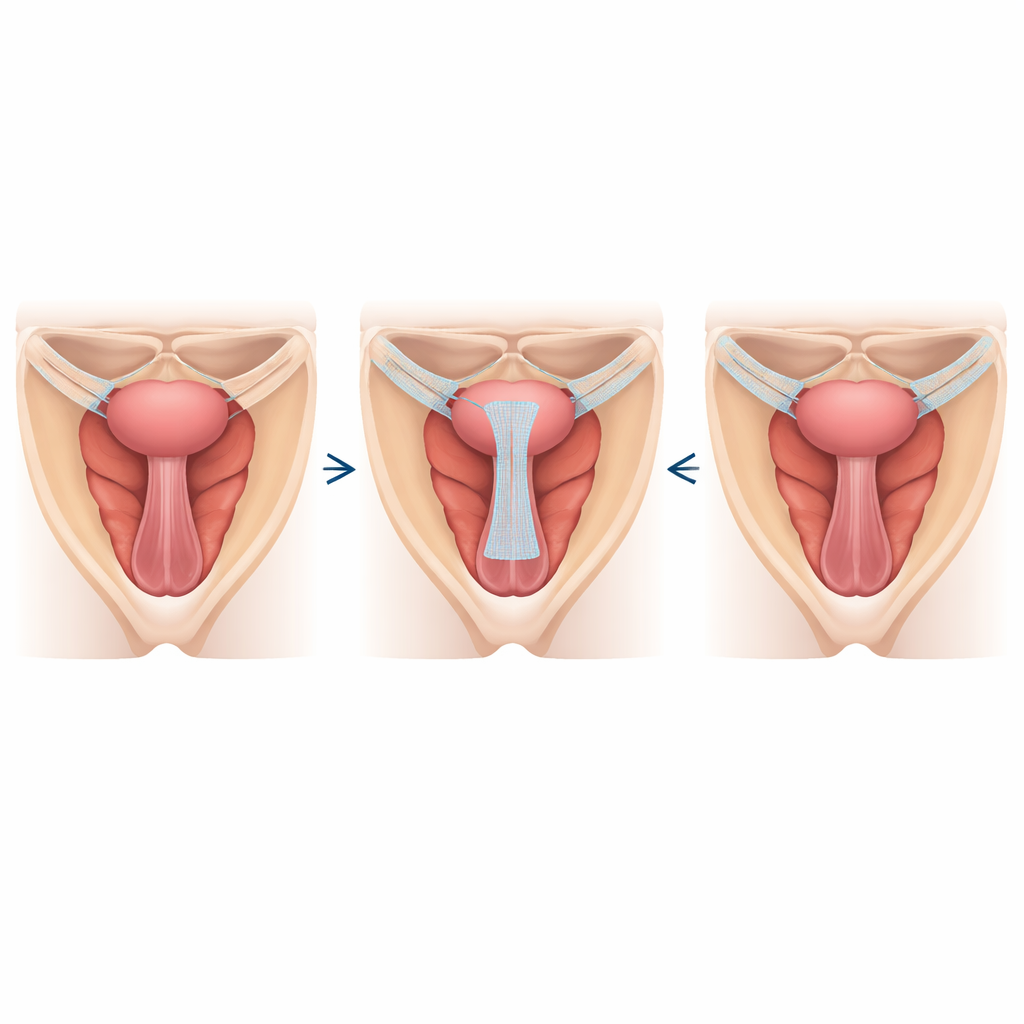
Traditional “gold standard” prolapse surgery anchors the top of the vagina or uterus to a strong ligament over the backbone, using surgical mesh. While effective, that route can be technically demanding and is not ideal for all women, especially those with scar tissue in the abdomen. Surgeons have recently developed an alternative route called pectopexy, which anchors mesh to two strong ligaments on either side of the front pelvic wall. Building on this idea, the team in this study designed an innovative version of pectopexy that uses an inverted T-shaped piece of mesh to support both the uterus (at the top) and the front vaginal wall (at the bottom) in a single operation. This design is meant to act like a hammock under the front of the vagina while also suspending the uterus in a natural position.
How the study was carried out
The researchers followed 67 women with advanced prolapse who chose keyhole reconstructive surgery at a single hospital between 2020 and 2023. Forty-two women, typically younger and more sexually active, had the new laparoscopic pectopexy with the T-shaped mesh and kept their uterus. Twenty-five women, often older or without significant front-wall prolapse, had the more established sacral procedure, where mesh is fixed to the backbone area. All surgeries were done by an experienced urogynecologist. Before and after surgery, the team measured the position of the pelvic organs, bladder function, bowel function, and sexual function using standard pelvic exams and detailed questionnaires. Women were then followed for one year to look for prolapse returning, symptoms, and any complications.
What the surgeons found
Both operations clearly helped. At one year, most women in both groups had their prolapse reduced to mild or none, and nearly all reported major improvements in pressure symptoms, bladder control, and daily comfort. Pain during sex decreased noticeably in women who had the new pectopexy, and no new cases of painful intercourse were reported in either group. Rates of common side effects, such as new urgency to urinate, were low and similar for the two operations, and no severe surgical complications occurred. However, when the researchers looked strictly at anatomy, the “cure” rate—defined as only very mild or no prolapse on exam—was somewhat lower with the new pectopexy (about 79%) than with the backbone-based surgery (about 92%).
Hidden weakness in the pelvic floor
To understand why prolapse recurred in some women, the team examined a range of factors, including age, body weight, childbirth history, heavy lifting, constipation, and previous prolapse operations. After careful statistical analysis, one factor stood out: damage to a key pelvic muscle group called the levator ani. In women with this kind of muscle detachment, the chance of prolapse coming back after the new pectopexy operation was much higher than in those with intact muscles. By contrast, whether a woman had the new or the standard operation did not, by itself, predict failure once muscle damage was taken into account. This suggests that the underlying strength of the pelvic floor may be more important than the choice of suspension technique when it comes to long-term support.
What this means going forward
For women with advanced prolapse who wish to preserve their uterus and need support for both the womb and the front vaginal wall, this pilot study suggests that the inverted T-mesh pectopexy is a promising, reasonably safe option with good symptom relief at one year. It may be especially appealing to younger, sexually active women because it restores support while maintaining the natural axis of the pelvis and avoids operating near the backbone and bowel. At the same time, the study highlights that serious weakness or tearing of key pelvic muscles greatly raises the risk of prolapse returning, no matter how clever the mesh design. Larger, longer-term studies are needed, but for now these results can help women and their surgeons have more informed, shared discussions about which prolapse surgery best suits their anatomy, lifestyle, and goals.
Citation: Yang, E., Tsai, CP., Shen, PS. et al. One-year outcomes of an innovative laparoscopic pectopexy procedure using inverted T-mesh for treatment of advanced uterine and anterior vaginal prolapse. Sci Rep 16, 11202 (2026). https://doi.org/10.1038/s41598-026-40730-0
Keywords: pelvic organ prolapse, uterine preservation surgery, laparoscopic pectopexy, pelvic floor muscles, surgical mesh