Clear Sky Science · en
Peripheral blood stem cells versus bone marrow graft for non-T-depleted haploidentical transplantation with post-transplant cyclophosphamide in patients with secondary acute myeloid leukemia in first complete remission: A study from the ALWP/EBMT
Why this research matters for patients
For many older adults, secondary acute myeloid leukemia is a life threatening blood cancer that often arises after years of other blood problems or chemotherapy. The only chance of long term control is usually a stem cell transplant, but many patients lack a perfectly matched donor. This study asks a practical question that directly affects real people and transplant centers worldwide: when using a half matched family donor and a modern drug strategy to control side effects, does it matter if doctors use stem cells collected from the bloodstream or from the bone marrow?
Two ways to collect life saving cells
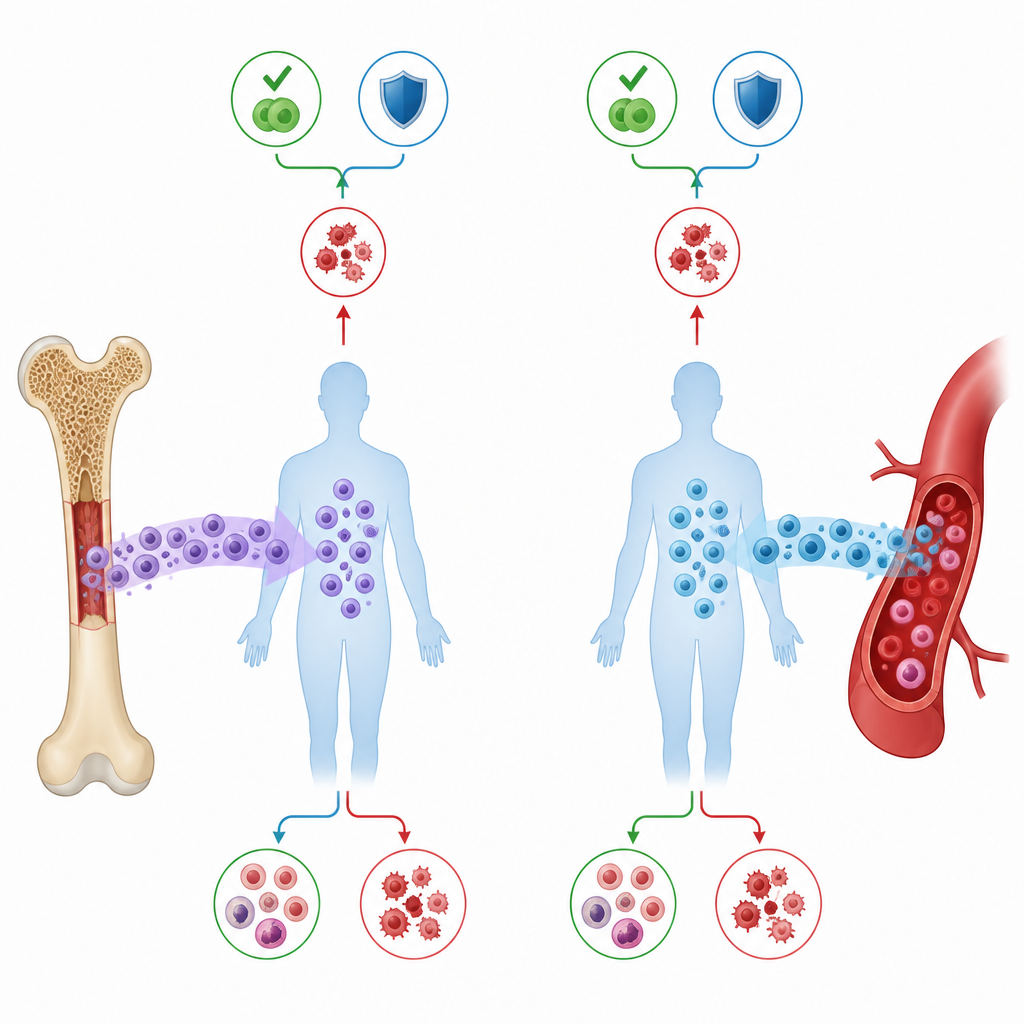
Doctors can obtain blood forming stem cells from a donor in two main ways. One is bone marrow, taken from the hip bones while the donor is under anesthesia. The other is peripheral blood stem cells, collected from the bloodstream after the donor receives a short course of medications that coax stem cells out of the marrow. Both sources can rebuild a patient’s blood system, but they differ in convenience, immune cell content, and the risk of complications such as graft versus host disease, where donor cells attack the patient’s tissues. In people with secondary acute myeloid leukemia, who are often older and medically fragile, choosing the safer and more effective option is especially important.
A large real world comparison
The researchers tapped into the European Society for Blood and Marrow Transplantation registry to look at 554 adults with secondary acute myeloid leukemia who received a first transplant from a half matched family donor between 2010 and 2021. All patients were in their first complete remission at the time of transplant and all received the same key drug strategy after transplant: high dose cyclophosphamide, which helps tame harmful immune reactions. Among them, 418 received peripheral blood stem cells and 136 received bone marrow. Apart from some differences in age and chemotherapy strength, the two groups were broadly similar in disease risk and general health.
What happened after transplant
The team tracked how quickly blood counts recovered, how often the cancer returned, deaths not related to relapse, and survival two years after transplant. They also measured acute and chronic graft versus host disease. Peripheral blood and bone marrow performed remarkably alike. Rates and timing of white cell and platelet recovery were close, and the chances of the leukemia returning were similar. Two years after transplant, overall survival hovered around 59 percent in both groups, and leukemia free survival was just above 50 percent. Serious complications such as fatal infections or organ damage occurred at comparable rates as well.
Other factors that shaped outcomes
While the choice of stem cell source did not change the big picture, other features clearly did. Patients with poorer performance status or a higher burden of other medical problems were more likely to die from causes other than relapse and had worse overall and leukemia free survival. Older age also increased the risk of non relapse death and chronic graft versus host disease. Unfavorable chromosome patterns in the leukemia cells raised the chance of relapse and shortened survival. A female donor for a male patient and older age were linked with more chronic graft versus host disease, again independent of whether stem cells came from blood or marrow.
What this means for patients and doctors
For adults with secondary acute myeloid leukemia receiving a half matched family transplant with post transplant cyclophosphamide, this study suggests that peripheral blood stem cells and bone marrow are equally valid choices. The main transplant outcomes, including survival and risk of relapse, were essentially the same for both graft types. That means doctors can base their decision on practical considerations such as donor comfort, collection logistics, and center experience, while focusing attention on factors that truly sway results, like overall fitness, other illnesses, and disease biology.
Citation: Nagler, A., Swoboda, R., Ferhat, AT. et al. Peripheral blood stem cells versus bone marrow graft for non-T-depleted haploidentical transplantation with post-transplant cyclophosphamide in patients with secondary acute myeloid leukemia in first complete remission: A study from the ALWP/EBMT. Bone Marrow Transplant 61, 559–568 (2026). https://doi.org/10.1038/s41409-026-02823-2
Keywords: stem cell transplant, secondary acute myeloid leukemia, haploidentical donor, peripheral blood stem cells, bone marrow graft