Clear Sky Science · en
Choroid plexus carcinoma: state of the field and emerging directions
Why this rare childhood brain cancer matters
Choroid plexus carcinoma is a rare but highly aggressive brain cancer that mostly strikes very young children, often before kindergarten. Because so few patients exist worldwide, there are limited data to guide doctors, and standard treatments can leave survivors with life‑long side effects. This review pulls together what scientists and clinicians now know about the disease, how it arises, how it is treated today, and how new lab models may finally open the door to safer, more precise care.
The brain’s fluid factory and how it goes wrong
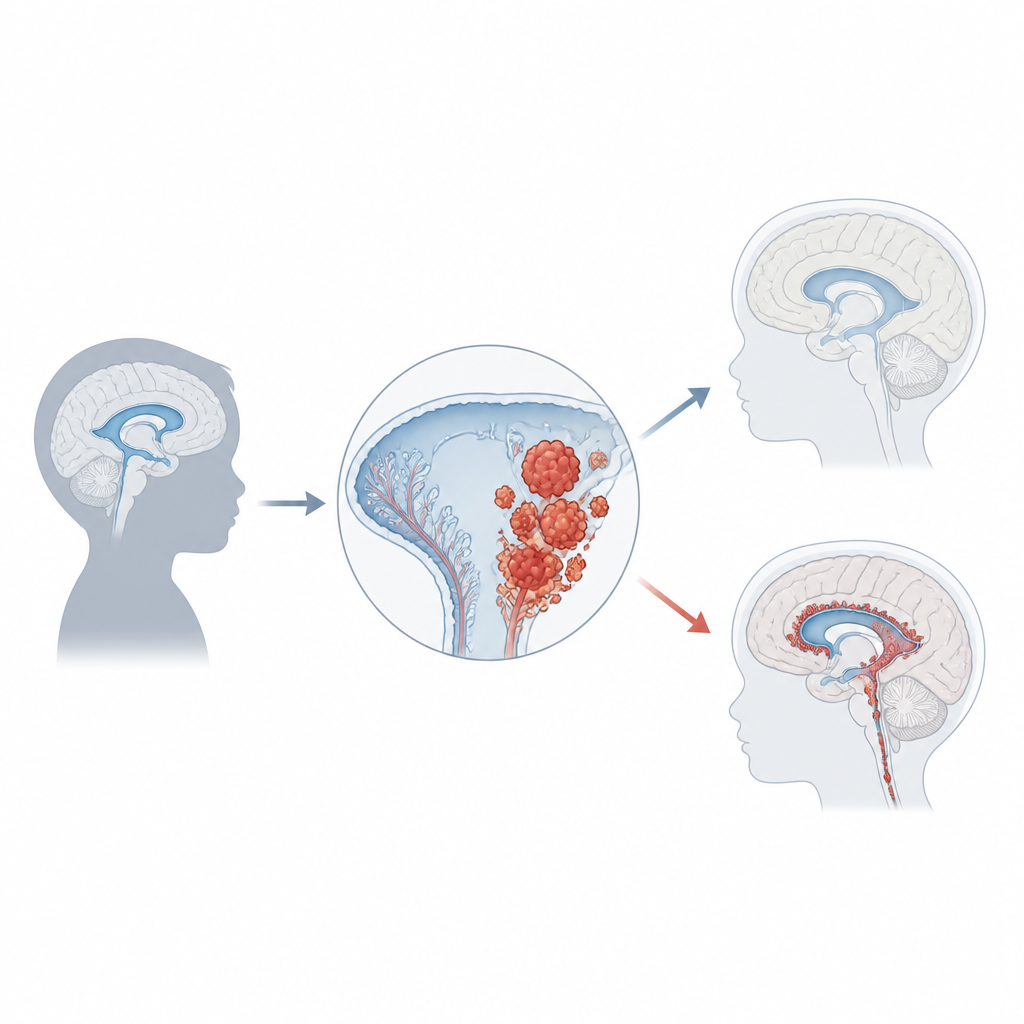
Deep inside each of the brain’s fluid‑filled spaces sits a thin, frilly tissue called the choroid plexus. Its main job is to produce cerebrospinal fluid, which cushions the brain and clears away waste. The tissue is made of specialized lining cells wrapped around tiny blood vessels and separated from the fluid by tight barriers. Unlike most nerve cells, choroid plexus cells can still divide slowly throughout life, which allows the tissue to repair itself after injury. That same capacity for growth, however, also makes it vulnerable to turning cancerous when key control genes are damaged.
A rare cancer with heavy impact on children
Choroid plexus carcinoma accounts for only about 1 percent of childhood brain tumors, but in babies under one year it can make up a fifth of all cases. Most children are diagnosed around age three, and the tumors usually arise in the side or back fluid spaces of the brain. As they grow, they often block the normal flow of fluid, leading to pressure build‑up called hydrocephalus. Families and doctors may first notice rapid head growth, vomiting, eye problems, headaches, seizures, or changes in behavior. Brain scans show large, irregular masses sprouting from the choroid plexus, but a firm diagnosis requires microscopic examination and modern molecular tests.
Genes, switches, and tumor risk
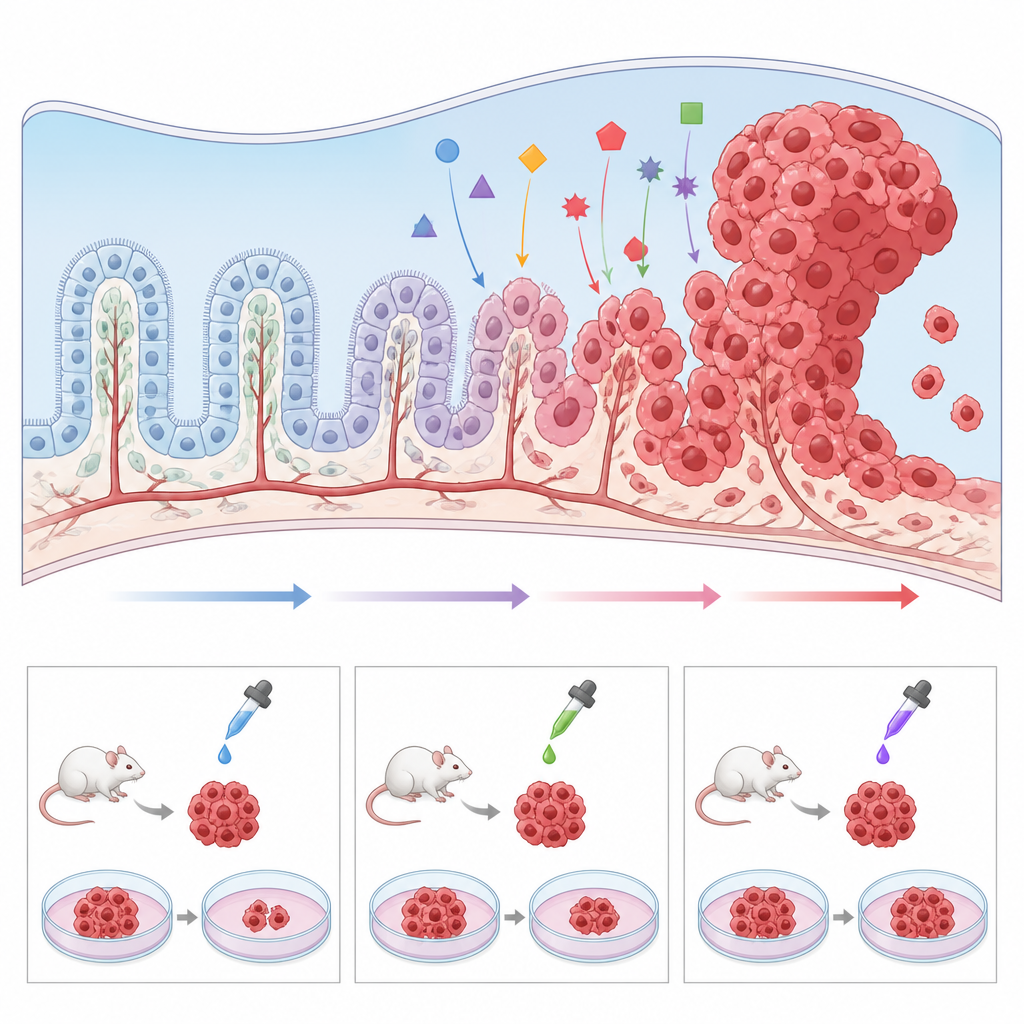
One of the strongest clues to how this cancer forms comes from genetics. Roughly half of tumors carry damage in TP53, a gene that normally halts growth or triggers cell death when DNA is harmed. Children who inherit TP53 mutations through Li‑Fraumeni syndrome are at especially high risk, and their tumors often carry many other DNA changes. These patients tend to fare worse than those whose TP53 remains intact. Other genes and pathways that push cells to grow or resist death, including MYC, Notch, and Wnt, are frequently disturbed as well. On top of DNA mutations, chemical tags on DNA that regulate gene activity form distinct “methylation” patterns, and one common pattern in these tumors correlates with more aggressive behavior. Together, these genetic and epigenetic fingerprints are beginning to sort patients into biologically meaningful subgroups.
How doctors treat it today
For now, the single most important factor linked to survival is how much of the tumor surgeons can safely remove. Children whose tumors are completely or nearly completely cut out do far better than those with large remnants. Because the cancer often spreads through the brain’s fluid pathways, many teams add chemotherapy and sometimes radiation after surgery. Yet radiation can seriously harm the developing brain, and it is particularly risky in children with TP53 mutations, who are prone to radiation‑induced second cancers. As a result, clinicians are testing combinations of intensive chemotherapy that aim to control the tumor while sparing or delaying radiation, especially in the youngest patients. Early results suggest that certain drug mixtures can help, but the best regimen likely depends on each tumor’s molecular profile.
Building better models in the lab
Because choroid plexus carcinoma is so rare, individual hospitals see very few cases, and tumor samples are scarce. To get around this obstacle, researchers are developing a suite of preclinical models. Genetically engineered mice that carry the same mutations found in children, such as TP53 loss and MYC activation, develop tumors in the same brain regions and allow careful study of how normal choroid plexus cells are pushed toward cancer. Tumor tissue can also be transplanted into mice or zebrafish to test drugs in a living system. In parallel, scientists have grown human tumor cell lines in dishes, as well as “mini choroid plexus” structures from stem cells, and have shown that tweaking pathways like Wnt can transform healthy‑like tissue into cancer‑like growths. These models make it possible to run high‑throughput screens of candidate drugs and to explore why some tumors resist standard therapy.
Looking ahead to more personal treatment
The article concludes that real progress against this childhood cancer will come from pairing careful genetic and epigenetic profiling of each patient’s tumor with powerful lab models that mirror those features. By learning which mutations, wiring changes, and cell types drive each case, researchers hope to match children to more tailored drug combinations and to design trials that avoid blanket use of harsh radiation. Although choroid plexus carcinoma will likely remain a rare disease, these emerging tools create a path toward longer survival and better quality of life for affected children.
Citation: Thompson, A., Pescaru, H., Griffin, B. et al. Choroid plexus carcinoma: state of the field and emerging directions. Oncogenesis 15, 21 (2026). https://doi.org/10.1038/s41389-026-00612-6
Keywords: choroid plexus carcinoma, pediatric brain tumor, TP53 mutation, brain cancer models, precision oncology