Clear Sky Science · en
Tripolar versus bipolar ablation: insights into lesion growth and geometry using a novel ablation approach for therapy-refractory ventricular arrhythmias
Why doctors are rethinking how they burn away dangerous heart rhythms
For some people with life‑threatening abnormal heart rhythms, standard treatments fail because the electrical trouble spot lies deep inside the heart wall, out of easy reach. This study explores a new way to deliver heat inside the heart more efficiently and safely, comparing a well‑established technique called bipolar ablation with a newer "tripolar" approach that adds a large grounding pad to help steer electrical energy. Understanding how these methods shape and grow the tiny burn marks they leave behind could one day make procedures for stubborn rhythm problems more effective and less risky.
Burning out bad circuits in the heart
When medicines and simpler procedures do not stop dangerous ventricular arrhythmias, doctors often turn to radiofrequency ablation. In this treatment, thin wires are threaded through blood vessels into the heart, where they deliver controlled heat to destroy misbehaving tissue. Traditional ablation sends current from a single catheter tip to a patch on the patient’s skin. Bipolar ablation, used for especially deep or hard‑to‑reach sites, instead sends current between two catheter tips pressed against opposite sides of the heart wall, creating a channel of heat between them. Yet this method can run into trouble if the electrical resistance between the catheters is high, limiting how much energy actually reaches the target and sometimes prompting operators to increase power, which raises the risk of explosive "steam pops" in the tissue.
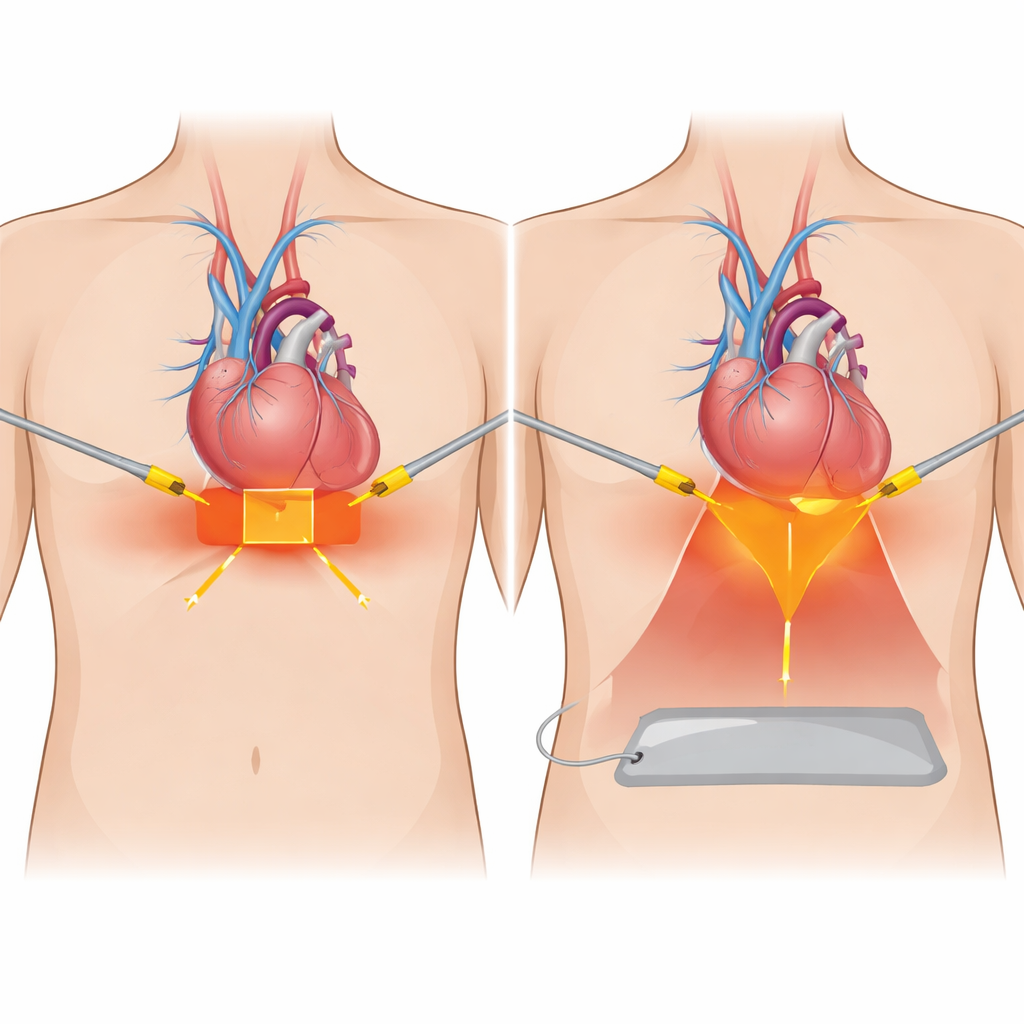
A new twist: adding a third path for current
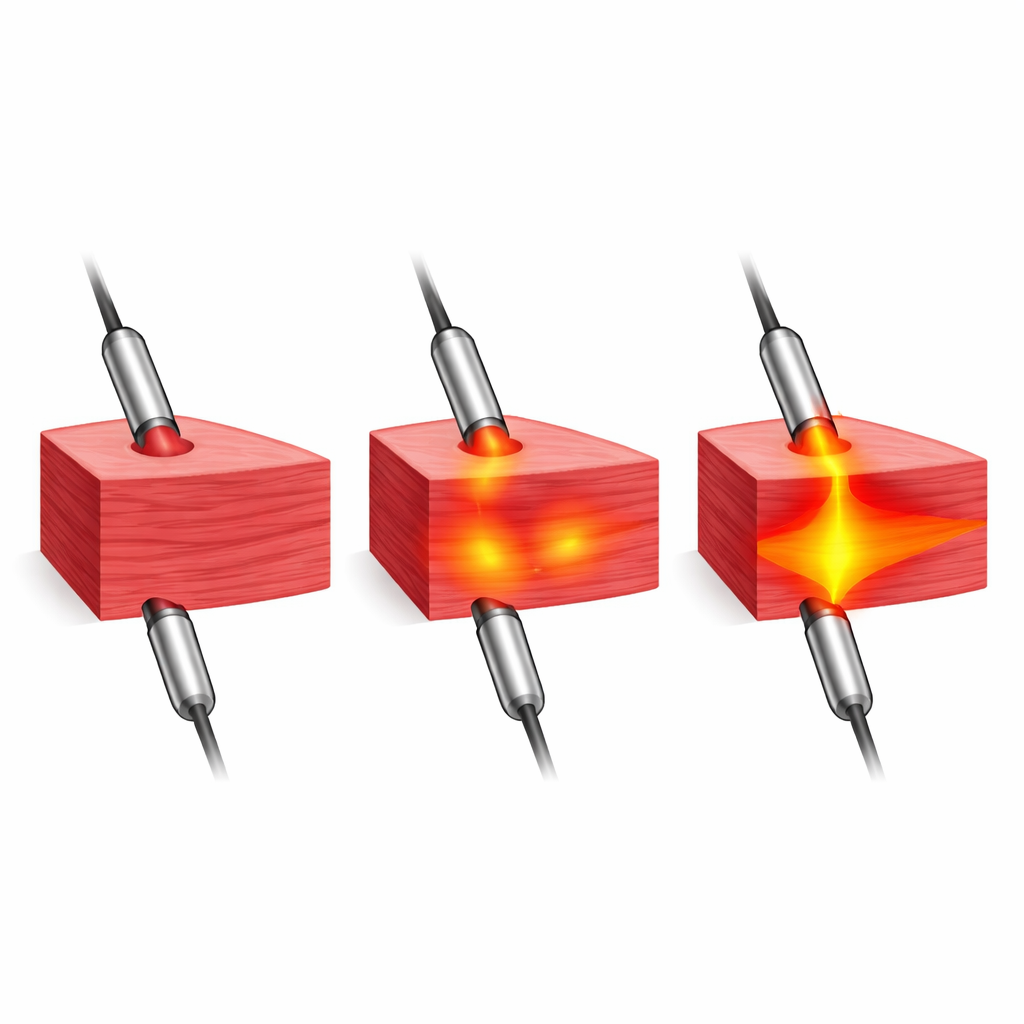
The researchers tested a modified setup they call tripolar ablation. It keeps the two opposing catheters of bipolar ablation but also connects a large dispersive pad beneath the heart slice as an extra pathway for current to leave the tissue. Working with cross‑sections of pig hearts kept warm in a saline bath, they applied carefully controlled bursts of energy at different power levels and filmed the resulting lesions second by second with a high‑resolution camera. This allowed them to measure how quickly each burn traveled through the wall, how deep and wide it became at each catheter tip, and how the overall volume of damaged tissue changed over time.
How lesion shape changes with an extra exit
Both methods were able to create full‑thickness burns across the heart wall in this model, but they did so in distinct ways. In classic bipolar ablation, the injuries at the two catheter tips looked almost like mirror images: similar depth and width, forming a nearly rectangular block of damaged tissue between them. In contrast, tripolar ablation produced a strikingly uneven pattern. The burn near the "active" catheter was clearly deeper and wider than the one at the opposite tip, giving the overall lesion a trapezoid‑like cross‑section that bulged toward the active side. Despite this shift, the total amount of damaged tissue at the moment the burn crossed the wall was similar between the two approaches.
Electrical resistance, timing, and safety
Adding the third pad in tripolar ablation reduced the starting electrical resistance compared with bipolar ablation, which can be helpful in clinical situations where resistance is unusually high and energy delivery is poor. However, tripolar lesions generally took somewhat longer to become full‑thickness, and in both techniques the burn continued to widen even after the tissue bridge had formed. Steam pops—sudden bursts caused by rapid boiling inside the muscle—appeared mostly at higher power settings (40 and 50 watts) and always after the lesion had already crossed the wall. Importantly, the frequency and timing of these pops were similar in both bipolar and tripolar setups, suggesting that the new configuration did not introduce obvious extra danger in this experimental context.
What this could mean for future heart procedures
For patients whose arrhythmia source sits deep within the heart or closer to one surface than the other, the asymmetrical lesions of tripolar ablation might offer a way to concentrate more damage where it is needed while sparing structures on the far side. At the same time, the continued growth of lesion width after full‑thickness damage is reached—and the clustering of steam pops at higher power—underline the need for careful control of energy and close monitoring of tissue heating. While this study was done in isolated pig hearts rather than living patients, it provides a detailed look at how an extra electrical pathway reshapes the burns created by ablation. The findings suggest that tripolar ablation could become a useful backup tool for particularly stubborn ventricular arrhythmias, provided its altered lesion geometry and safety profile are confirmed and refined in future clinical research.
Citation: Bahlke, F., Abdiu, E., Schultz, E. et al. Tripolar versus bipolar ablation: insights into lesion growth and geometry using a novel ablation approach for therapy-refractory ventricular arrhythmias. Sci Rep 16, 12739 (2026). https://doi.org/10.1038/s41598-026-48782-y
Keywords: ventricular arrhythmia, radiofrequency ablation, bipolar ablation, tripolar ablation, cardiac electrophysiology