Clear Sky Science · en
Skull base reconstruction strategy for high-flow CSF leaks during EEA surgery based on the quality of pedicled nasoseptal flap
Protecting the Brain’s Hidden Gateway
The floor of the skull is a delicate gateway between the clean, fluid-filled space around the brain and the bacteria-filled airways of the nose. Modern surgeons often reach deep-seated brain tumors through the nostrils using an endoscope, but this route can leave a leaky opening in that barrier. The study summarized here explores how best to patch this opening so that brain fluid does not seep into the nose and cause dangerous infections.
Why Nose-Based Brain Surgery Risks a Leak
Endoscopic endonasal surgery lets doctors remove tumors near the pituitary gland and surrounding region through natural nasal passages instead of opening the skull. While this approach avoids a large external incision and can improve recovery, it also punctures the thin walls that normally keep cerebrospinal fluid (the clear liquid bathing the brain) completely separate from the nasal cavity. When that fluid escapes quickly during surgery, the leak can be difficult to control and, if not repaired well, can later lead to fluid dripping from the nose, severe headaches, and serious infections like meningitis.
Using Living Nasal Tissue as a Natural Patch
To plug these openings, surgeons commonly use a piece of living tissue from inside the nose called a pedicled nasoseptal flap. This flap is cut from the nasal septum but left attached to its blood supply, so it behaves like a living bandage. In this study, the team focused on how the condition of that flap—its size, thickness, and blood flow—should influence the repair strategy. They examined 86 patients who had strong, moderate, or unusable flaps and compared how well different multi-layer repair plans protected against leaks and infections after surgery.
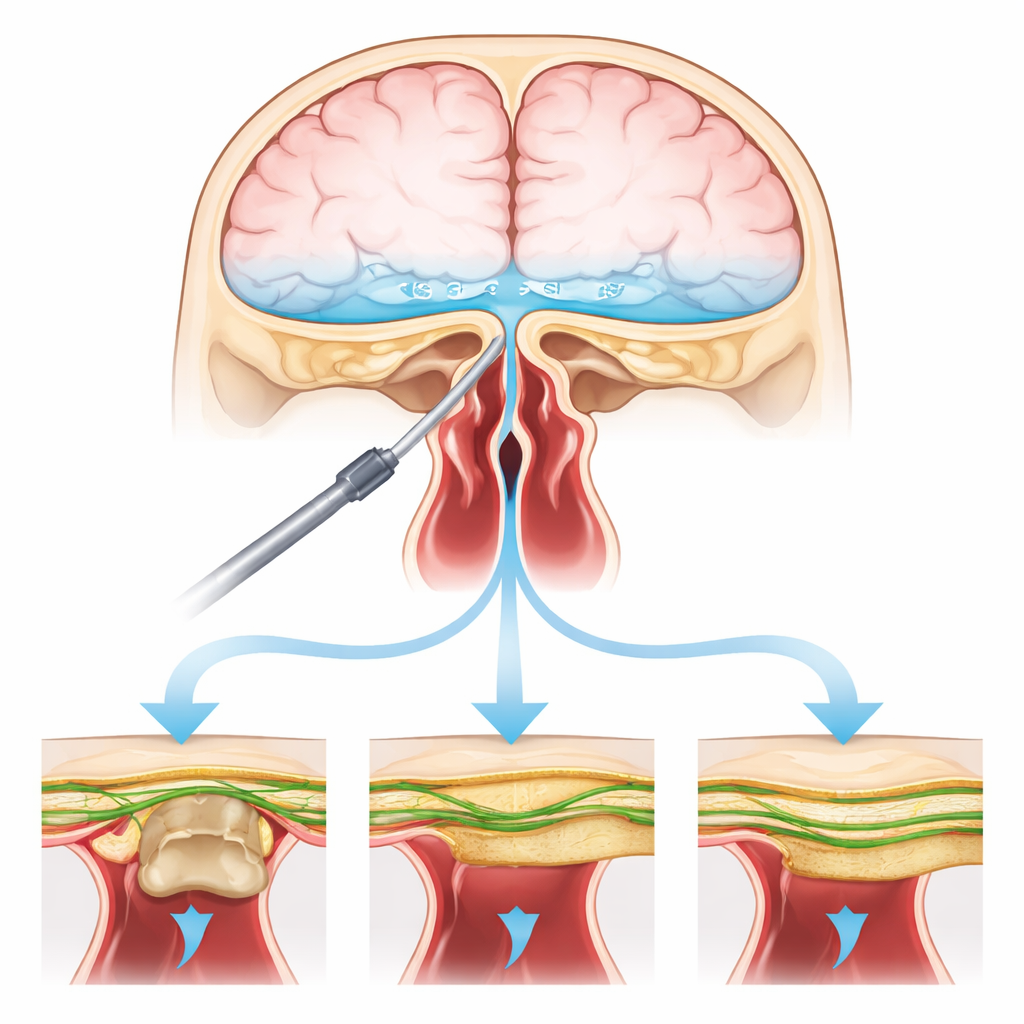
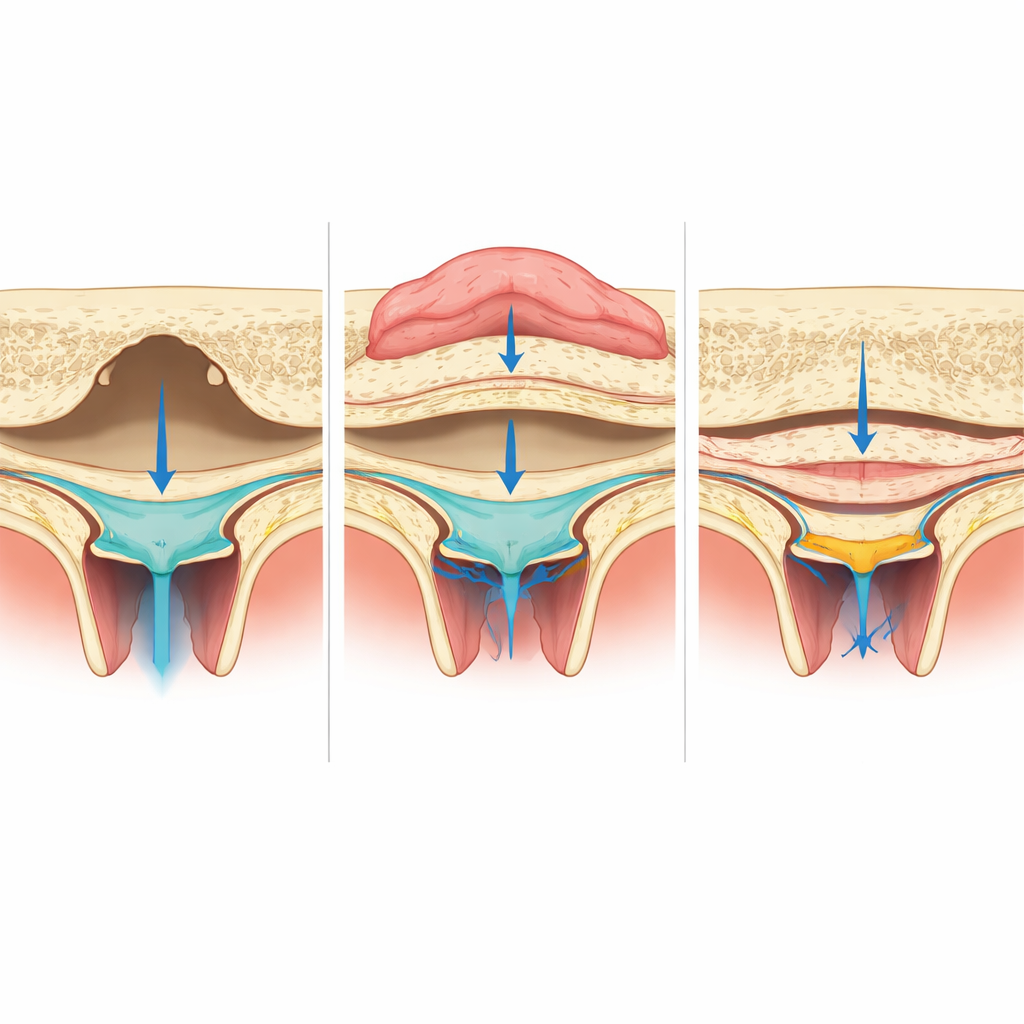
Three Repair Plans for Three Tissue Qualities
The researchers grouped patients into three categories. In the first group, the flap was large, intact, and well supplied with blood. Surgeons first placed a thin artificial membrane beneath the brain lining, then restored a piece of bone over the opening, and finally draped the healthy flap over everything like a roof. In the second group, the flap was somewhat damaged or showed signs of poor circulation. Here, an extra strip of strong connective tissue taken from the thigh (fascia lata) was added on top of the membrane to reinforce the seal before the nasal flap was laid over it. In the third group, the flap was too damaged to rely on, so surgeons built the repair mainly from layers of thigh tissue, sometimes combined with a fat plug, to recreate a sturdy barrier in place of the nasal flap.
Outcomes: Fewer Leaks, Fewer Infections
Across all 86 patients, the tailored, layered repairs worked well. Only three people (3.5%) developed a new leak after surgery, and four (4.7%) developed meningitis—rates lower than those often reported in similar operations. Importantly, complication rates were similar in all three groups, suggesting that when the nasal flap is poor or absent, a carefully planned fascia-based reconstruction can still protect the brain effectively. However, patients whose nasal flap could not be used had to stay in bed and in the hospital noticeably longer, likely because their repairs relied on tissue without its own blood supply and took more time to fully heal.
What This Means for Patients
This work shows that there is no one-size-fits-all patch for closing the skull base after nose-based brain surgery. Instead, surgeons should judge the condition of the nasal flap and then choose the repair recipe—living flap, bone, thigh tissue, fat, or combinations—that best recreates the skull’s natural layers. A healthy, well-perfused nasal flap remains the ideal outer shield, especially when supported by restored bone. When that flap is weak or missing, thoughtfully stacked layers of graft tissue can still keep brain fluid where it belongs and lower the chance of dangerous leaks and infections. For patients, this means that even in challenging situations, a personalized reconstruction plan can make this minimally invasive route to deep brain tumors both safer and more reliable.
Citation: Fu, YH., Wu, XQ., Luo, YW. et al. Skull base reconstruction strategy for high-flow CSF leaks during EEA surgery based on the quality of pedicled nasoseptal flap. Sci Rep 16, 12782 (2026). https://doi.org/10.1038/s41598-026-43689-0
Keywords: cerebrospinal fluid leak, endonasal skull base surgery, nasoseptal flap, skull base reconstruction, pituitary region tumors