Clear Sky Science · en
“Fate of pressure-bearing flaps: long-term observations”
Why the Bottom of the Foot Matters
For people who have serious wounds on their feet—often from diabetes, injuries, or poor circulation—modern surgery can move healthy tissue from one part of the body to cover damaged areas and save the limb. But even when these transplanted tissue patches, called flaps, survive, doctors still worry about a later problem: new sores that form where the foot has to bear weight every day. This study followed patients for several years after such reconstructive surgery to learn exactly where on the foot these ulcers are most likely to return, and what that means for long-term walking and limb health.
How Surgeons Rebuild a Damaged Foot
When a wound on the foot is too large or too deep to heal on its own, surgeons may perform free-flap surgery. They move a piece of skin, fat, and sometimes muscle—along with its blood vessels—from another body area and connect it to vessels in the foot under a microscope. This creates a fresh, well‑supplied cover over exposed bone or tendon and can prevent amputation. In this study, 90 patients who had such surgery between 2015 and 2022 were followed for at least two years. Their wounds came from diabetes‑related ulcers, accidents, infections, or cancer removal, and most had serious underlying problems such as poor circulation, bone infection, or kidney failure.
Different Jobs for Different Parts of the Foot
The researchers divided the foot into broad regions to understand how daily forces affect the new tissue. The underside, or plantar surface, is where the body’s weight is carried, especially under the forefoot and heel. The top, or dorsal surface, does not press directly against the ground but can still rub against shoes. To get more detail, the team further split the foot into seven smaller zones—such as the inner and outer parts of the forefoot, the middle of the sole, and the heel—reflecting how pressure shifts while walking. They then tracked where ulcers appeared on the flaps, how deep they went, how often they came back, and whether patients eventually needed more surgery or even amputation.
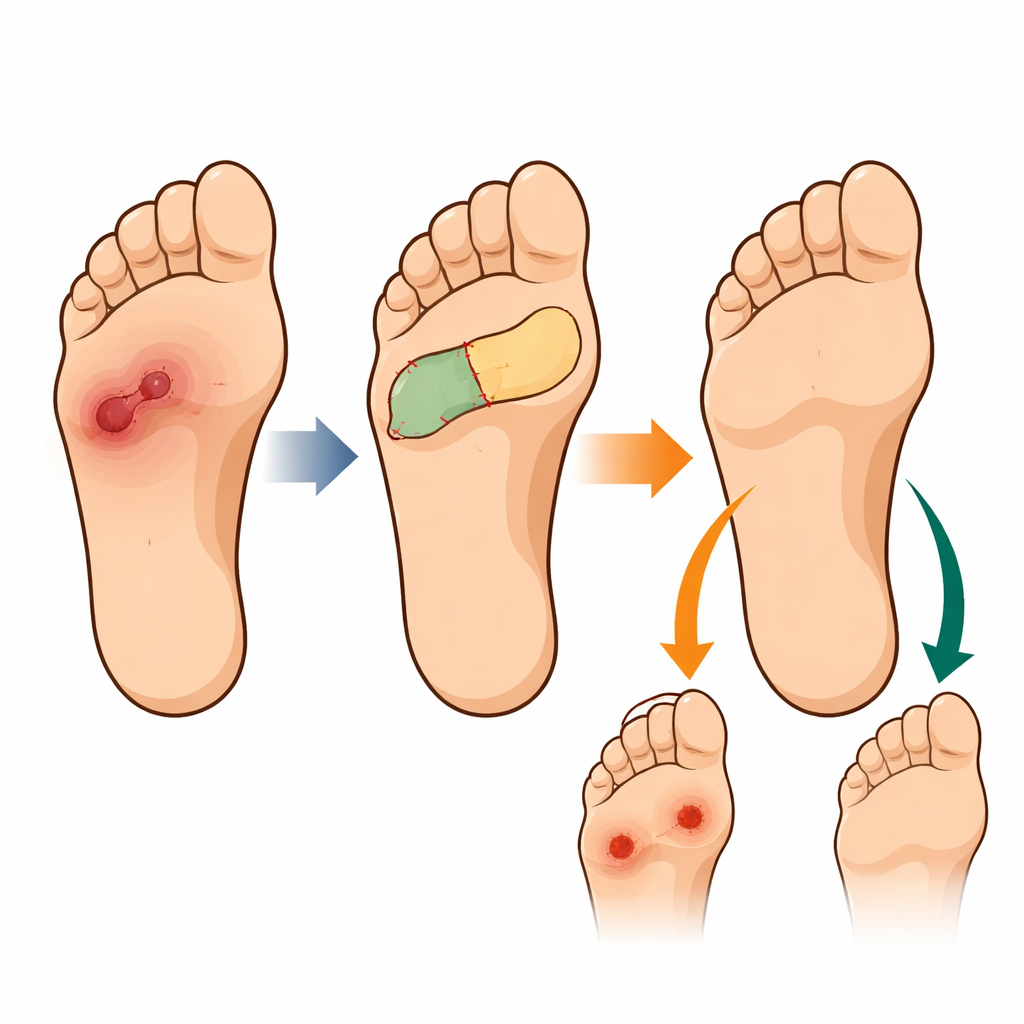
Where Trouble Shows Up After Surgery
Although the flaps themselves survived in more than 93 percent of patients, new ulcers still developed in nearly one in three. Location turned out to be crucial. When the flap was on the bottom of the foot, ulcers were far more common: about 43 percent of plantar flaps broke down, compared with only about 10 percent of flaps on the top of the foot. Sores on the underside appeared later—on average about eight and a half months after surgery—tended to recur almost three times per patient, and were often deep enough to involve bone. Many of these required additional surgery, and three patients ultimately needed below‑knee amputations. In contrast, ulcers on the top of the foot showed up earlier, were milder, usually healed with careful wound care and shoe adjustments, and never led to limb loss.
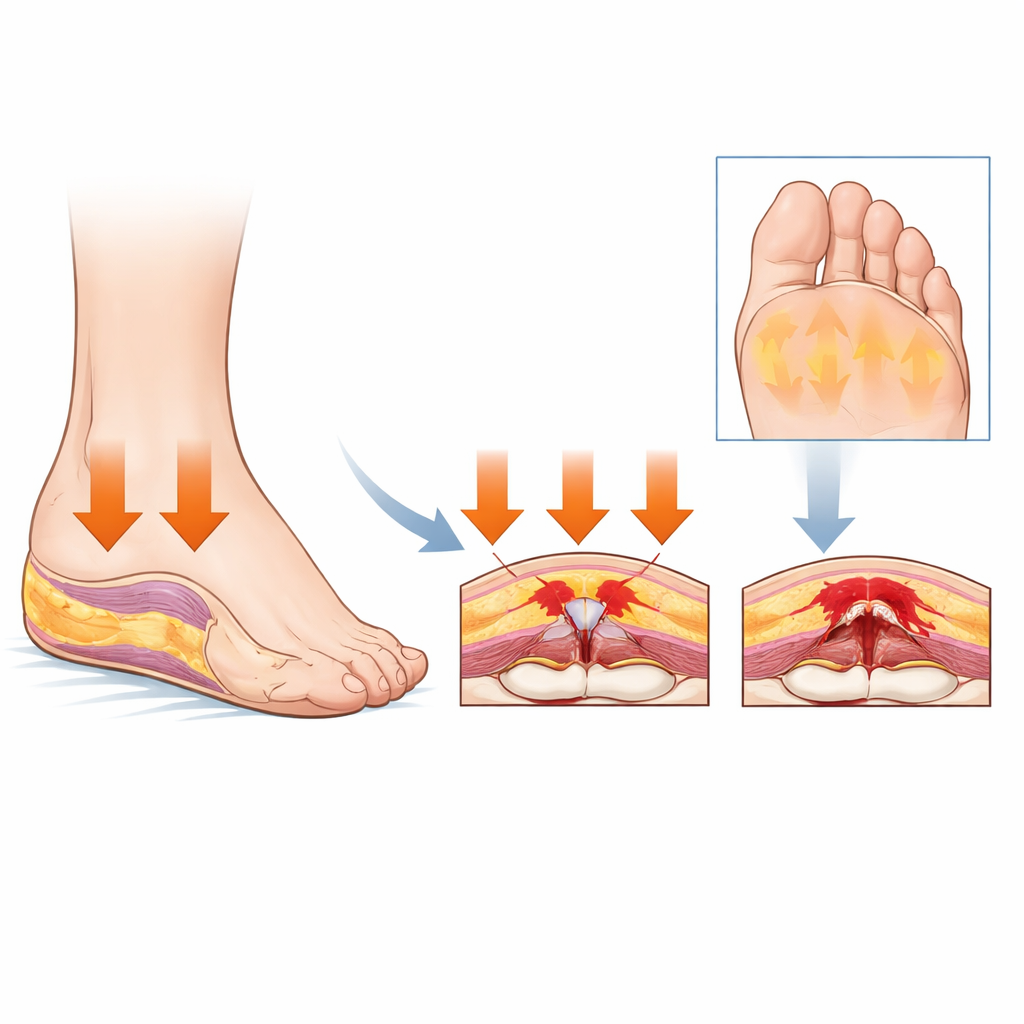
The Forefoot Takes the Hardest Hit
Digging deeper into the anatomy, the study showed that the front part of the sole, where the toes push off the ground, was the most fragile area after reconstruction. Flaps covering the inner and outer forefoot were especially likely to ulcerate and did so sooner than other regions. Statistical models that accounted for diabetes, bone disease, flap size, and blood‑vessel procedures all pointed to the same message: simply being on the weight‑bearing underside of the foot, especially the forefoot, greatly increased long‑term ulcer risk. Other technical details of the surgery—such as flap type, size, or which artery was used—did not meaningfully change that risk.
What This Means for Patients and Care Teams
For patients, the core message is that saving the foot with advanced surgery is only the beginning. When reconstruction involves the sole—particularly the front of the foot—the new tissue lives under constant pounding and sliding forces with every step. This study shows that those regions remain vulnerable to serious, sometimes limb‑threatening sores for many years. For surgeons and rehabilitation teams, it underscores the need to choose flap designs that match the mechanical demands of the plantar surface, to provide tailored footwear and pressure‑relieving devices, and to maintain long‑term follow‑up. With thoughtful planning and ongoing monitoring, the chances of keeping a reconstructed foot both intact and comfortable over the long haul can be significantly improved.
Citation: Lee, Mk., Park, B.Y. “Fate of pressure-bearing flaps: long-term observations”. Sci Rep 16, 12408 (2026). https://doi.org/10.1038/s41598-026-42611-y
Keywords: foot reconstruction, pressure ulcers, diabetic foot, plantar forefoot, free flap surgery