Clear Sky Science · en
The progressive journey of poor-responder neovascular AMD: tracking structural evolution and visual decline over time
Why some treated eyes still lose sight
For many older adults, injections of anti-VEGF drugs into the eye have been a lifeline, slowing or stopping vision loss from a severe form of age-related macular degeneration (AMD). Yet a sizable group of patients continues to lose vision even while faithfully receiving treatment. This study follows those "poor-responder" eyes over several years, revealing what is really happening inside the central retina and why standard scans can give a false sense of security.
Looking beyond thickness on eye scans
Eye doctors usually track the success of anti-VEGF therapy by measuring the thickness of the central retina on optical coherence tomography (OCT) scans. Thicker tissue is often interpreted as swelling and active disease; thinner tissue is seen as improvement. The authors suspected this simple measure was missing a more complex story. They focused on patients whose vision dropped by at least 10 letters on a standard eye chart despite multiple injections and apparently good control of retinal thickness. In 70 such eyes, they examined high-resolution OCT scans and vision tests at three key moments: soon after the first injection series, when that 10-letter loss first appeared, and when vision reached its worst point during follow-up.
Three stages in a slow decline
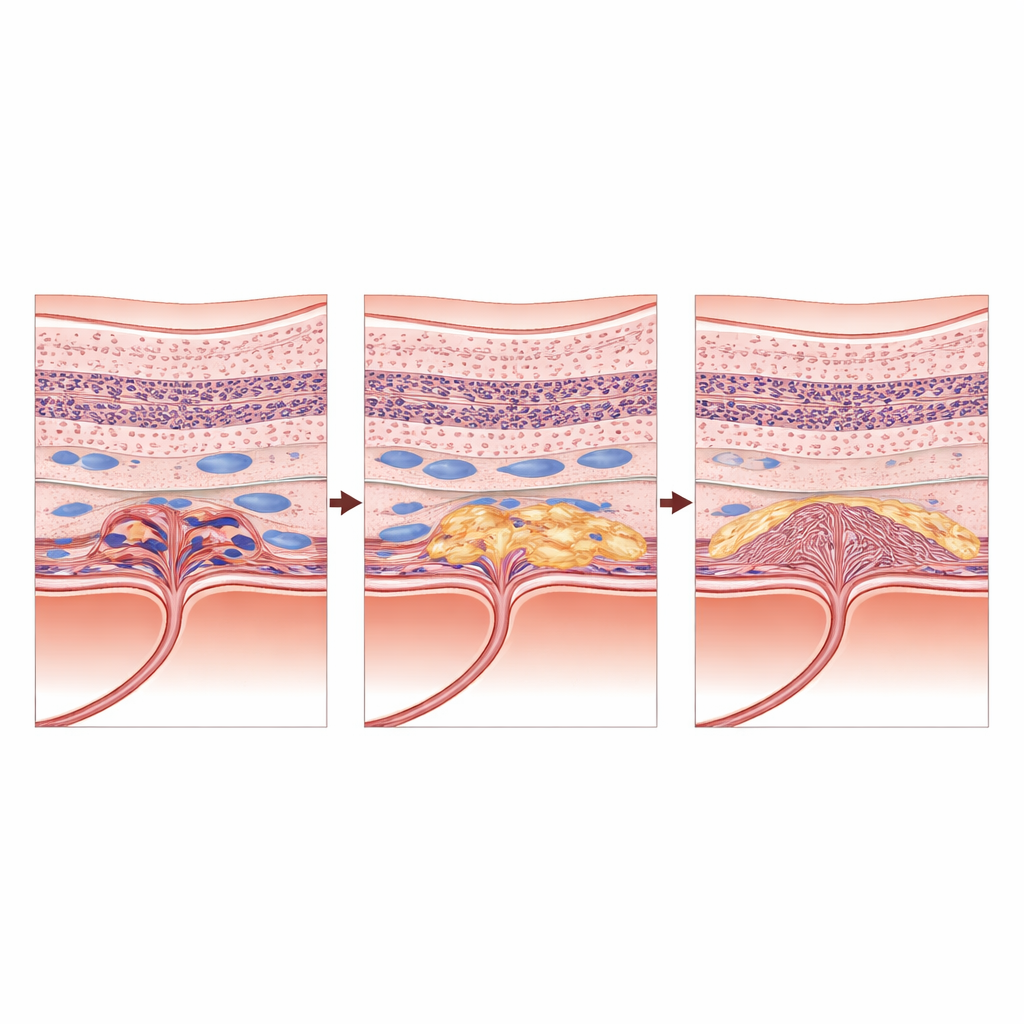
The team found that the structure of the central retina in these poor-responder eyes changed in a characteristic three-phase journey. At the first timepoint, after initial treatment, vision and structure appeared relatively stable, and no single feature on the scans clearly predicted how well patients would see. By the time each eye lost 10 letters of vision, however, several damaging changes had emerged together. Many eyes had begun to develop patches of macular atrophy—areas where the light-sensing cells and their support layer were permanently lost. At the same time, more eyes showed subretinal fibrosis, a scar-like tissue growing beneath the retina, and subtle deposits of hyperreflective material. Intraretinal fluid pockets within the retinal tissue also persisted. Vision at this middle stage was best explained by a combination of these changes, especially the early scarring under the retina.
Scarring takes control
As years passed, the disease picture became dominated by permanent damage. Macular atrophy rose from 7 percent of eyes after the first injections to over 80 percent at the worst-vision visit. Subretinal fibrosis climbed from about 11 percent to more than half of the eyes. By that final stage, a single factor stood out: subretinal fibrosis alone best explained how poor vision had become, overshadowing even the extensive atrophy. In other words, once a dense scar formed beneath the macula, it became the main determinant of sight, and other features added little further information about visual performance.
When shrinking on a scan is bad news
One of the most striking findings was that central retinal thickness, the standard metric used worldwide to guide treatment, did not predict vision at any stage. Thickness followed a puzzling pattern: it first increased slightly around the time of the 10-letter loss, then decreased again as vision worsened. Rather than reflecting healing, that later thinning likely marked ongoing loss of retinal tissue. Eyes could look "better" numerically while silently accumulating scarring and atrophy. Fluid beneath the retina gradually resolved in many patients, which might appear reassuring on routine review, yet intraretinal fluid remained common and turned out to be an independent warning sign of future visual decline at the middle timepoint.
What this means for patients and doctors
For people living with neovascular AMD, this study explains why vision may continue to fade despite regular injections and "good"-looking thickness numbers. Poor-responder eyes seem to pass through a critical window, when inflammation, leaking vessels, and early scarring act together to damage the macula, before entering a stage where scar tissue rules and treatment options are limited. The authors argue that care must shift from simply tracking how thick the retina is to carefully examining the quality of its structure: the growth of scar tissue, the spread of atrophy, and the presence of fluid within the tissue. In the future, smarter imaging tools and artificial intelligence may help doctors detect these warning signs earlier and tailor more aggressive or combined treatments. Ultimately, the work calls for a change in mindset—away from a single number on a scan and toward a richer, scar-focused view of what truly threatens sight.
Citation: Lolli, I., Pignataro, M.G., Termite, A.C. et al. The progressive journey of poor-responder neovascular AMD: tracking structural evolution and visual decline over time. Eye 40, 827–834 (2026). https://doi.org/10.1038/s41433-026-04306-6
Keywords: age-related macular degeneration, anti-VEGF treatment, retinal scarring, optical coherence tomography, vision loss progression