Clear Sky Science · en
Acute coronary syndromes across the lifespan of women
Why this topic matters to women and their families
Heart attacks are often seen as a man’s disease, yet they are a leading cause of illness and death for women of all ages. This article explains how heart attacks and related emergencies, grouped under the term acute coronary syndromes, can look different in women than in men, why those differences matter, and how a woman’s risk changes from childhood through older age. Understanding these patterns can help women, their families, and their clinicians recognize warning signs earlier and choose care that fits women’s unique needs.
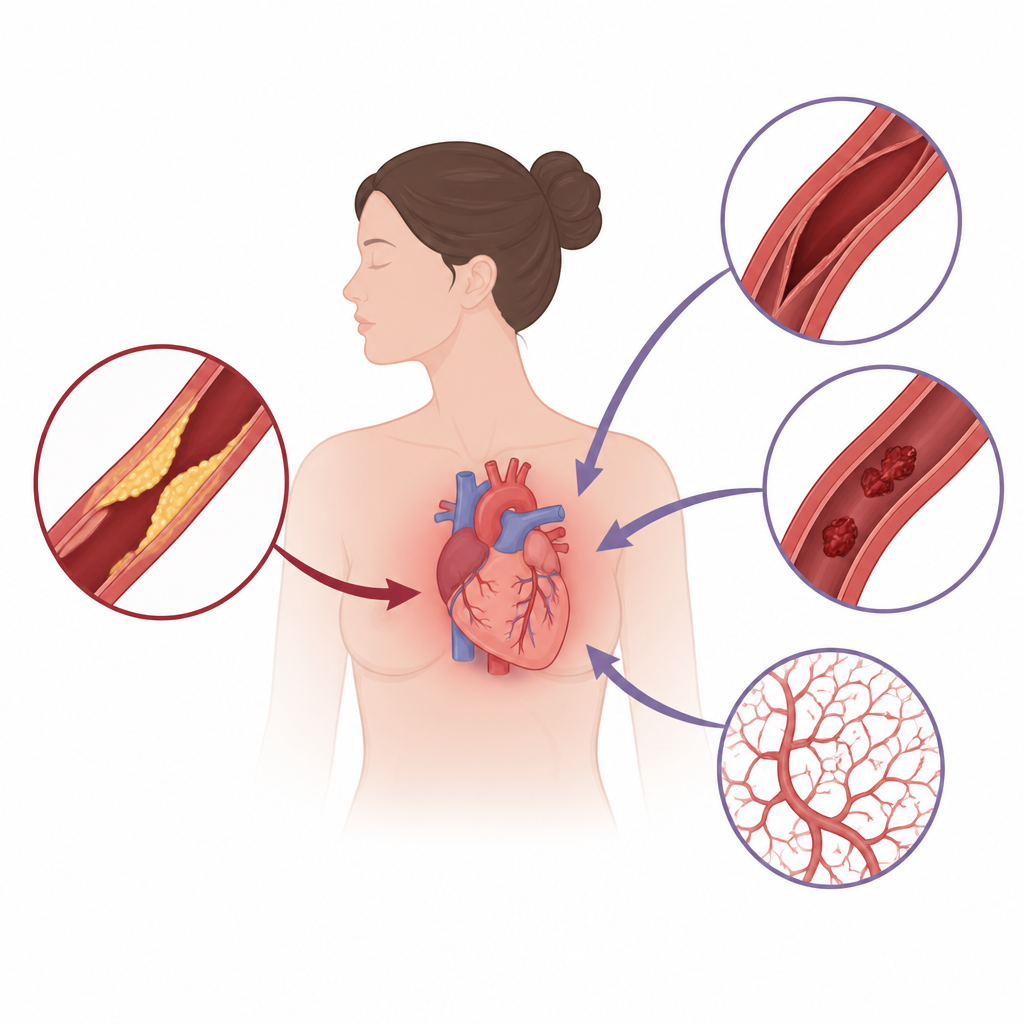
Different heart troubles in women
For many years, most heart research focused on men, so doctors were taught to look for the classic image of a middle aged man clutching his chest. The authors show that women’s heart events often follow different paths. Women are more likely than men to have heart attacks without major artery blockages, caused instead by vessel spasms, small vessel problems, tears in the artery wall, or clots that travel from elsewhere. Their symptoms may involve chest pain but also shortness of breath, exhaustion, nausea, or confusion, especially at younger and older ages. Because these patterns fall outside the traditional script, women are more likely to be misdiagnosed, treated later, or not offered the same tests and procedures as men.
Life stages and changing risk
The authors organize women’s heart risk across the lifespan. In childhood and adolescence, problems such as congenital heart defects, rare inflammatory illnesses, and early exposure to tobacco, vaping, or stimulants can quietly shape later risk. In reproductive years, heart attacks remain uncommon but become more tied to factors that mainly affect women, including pregnancy, autoimmune diseases, and a condition called spontaneous coronary artery dissection, in which the wall of a heart artery splits. During pregnancy and the months after delivery, the circulation is under extra strain, blood becomes more prone to clotting, and serious complications of pregnancy are linked to a higher chance of heart disease many years later.
Midlife changes and hidden warning signs
As women enter their 40s, 50s, and early 60s, the shift into menopause plays a central role. Falling estrogen levels are linked to stiffer blood vessels, higher blood pressure, unfavorable cholesterol changes, and weight gain around the abdomen. Some women experience chest pain or breathlessness despite having little or no visible blockage in the main heart arteries, reflecting problems in the smaller vessels that are harder to detect with standard tests. Cancer treatments, especially for breast cancer, can also injure the heart and arteries and may not be recognized as a heart risk for years. Traditional factors such as high blood pressure, diabetes, smoking, and inactivity are especially harmful to women, often raising their relative risk more than in men.
Later years and added challenges
In older age, clogged heart arteries become more common in women, but their heart attacks often present with vague symptoms such as weakness, confusion, or shortness of breath rather than dramatic chest pain. Many older women live with multiple health problems, frailty, and long lists of medications, which raise the risk of bleeding and complications from invasive procedures. They are still less likely than men to receive quick artery opening treatments or full-strength prevention medicines. Social factors, including living alone, caregiving duties, financial strain, and experiences of racism or discrimination, also shape risk and access to care for many women across racial and ethnic groups.
Steps toward fair and tailored heart care
The review concludes that heart emergencies in women arise from a mix of sex specific biology, life events such as pregnancy and menopause, social stressors, and uneven healthcare. Because risk factors and disease mechanisms shift over time, the authors argue for a lifespan approach that starts with early awareness in girls, includes pregnancy history as a routine heart risk signal, and adapts testing and treatment to women’s ages and circumstances. They call for more research that includes women of all backgrounds, better recognition of subtle symptoms, thoughtful use of blood thinners and other drugs, and greater referral of women to cardiac rehabilitation. Taken together, these steps could make heart care more accurate, timely, and equitable for women throughout their lives.
Citation: Donisan, T., Hagan, G., Tweet, M.S. et al. Acute coronary syndromes across the lifespan of women. npj Cardiovasc Health 3, 26 (2026). https://doi.org/10.1038/s44325-026-00126-5
Keywords: women’s heart disease, acute coronary syndrome, pregnancy and heart risk, menopause and heart health, microvascular angina