Clear Sky Science · en
Percutaneous Coronary Intervention and vascular access complications: A contemporary review
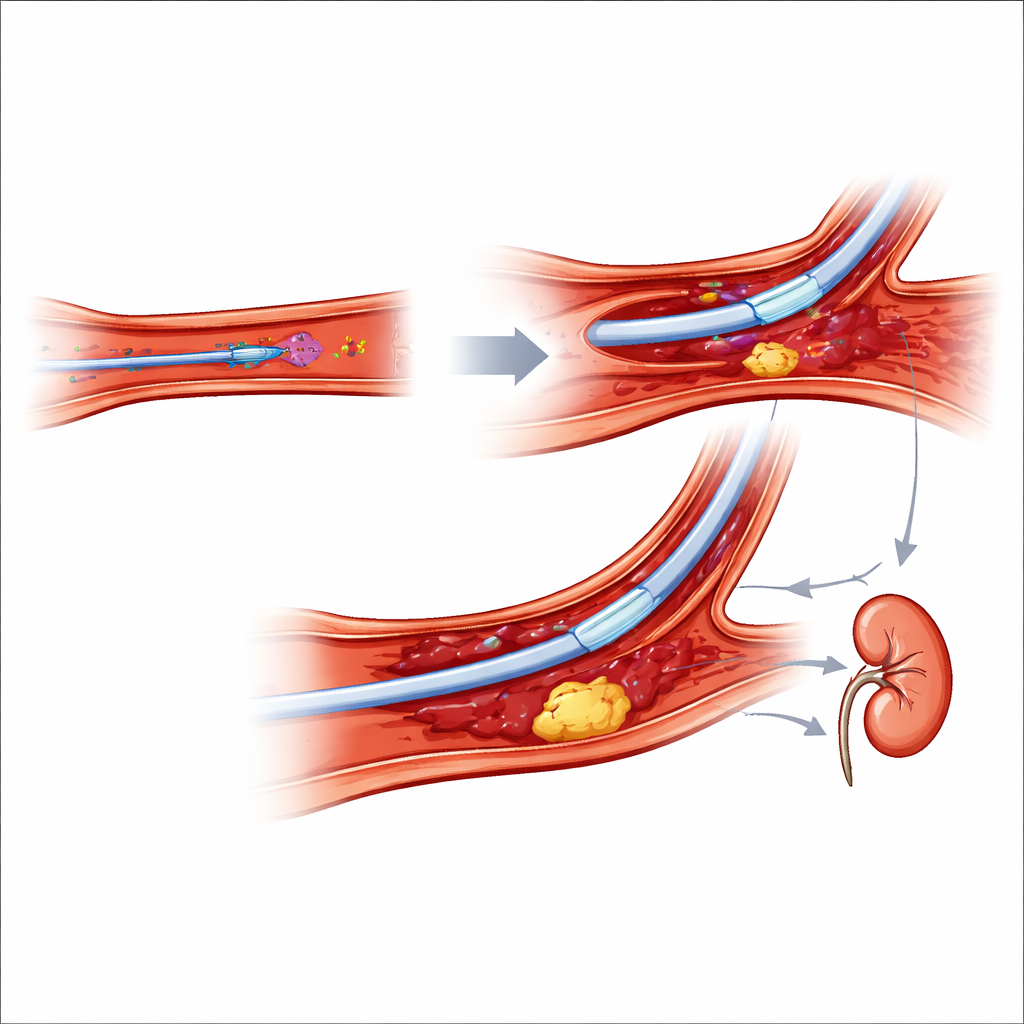
Why the Way to the Heart Matters
Heart doctors often reach clogged arteries not by opening the chest, but by guiding thin tubes through blood vessels from the wrist or the groin. This article explains why choosing the wrist (the transradial approach) has become the preferred route over the groin (the transfemoral approach), how each path can go wrong, and what doctors are doing to keep these life‑saving procedures as safe as possible. Understanding these trade‑offs helps patients know what to ask before a stent or coronary angiogram and why the spot where the tube goes in can affect bleeding, kidney health, and even survival.
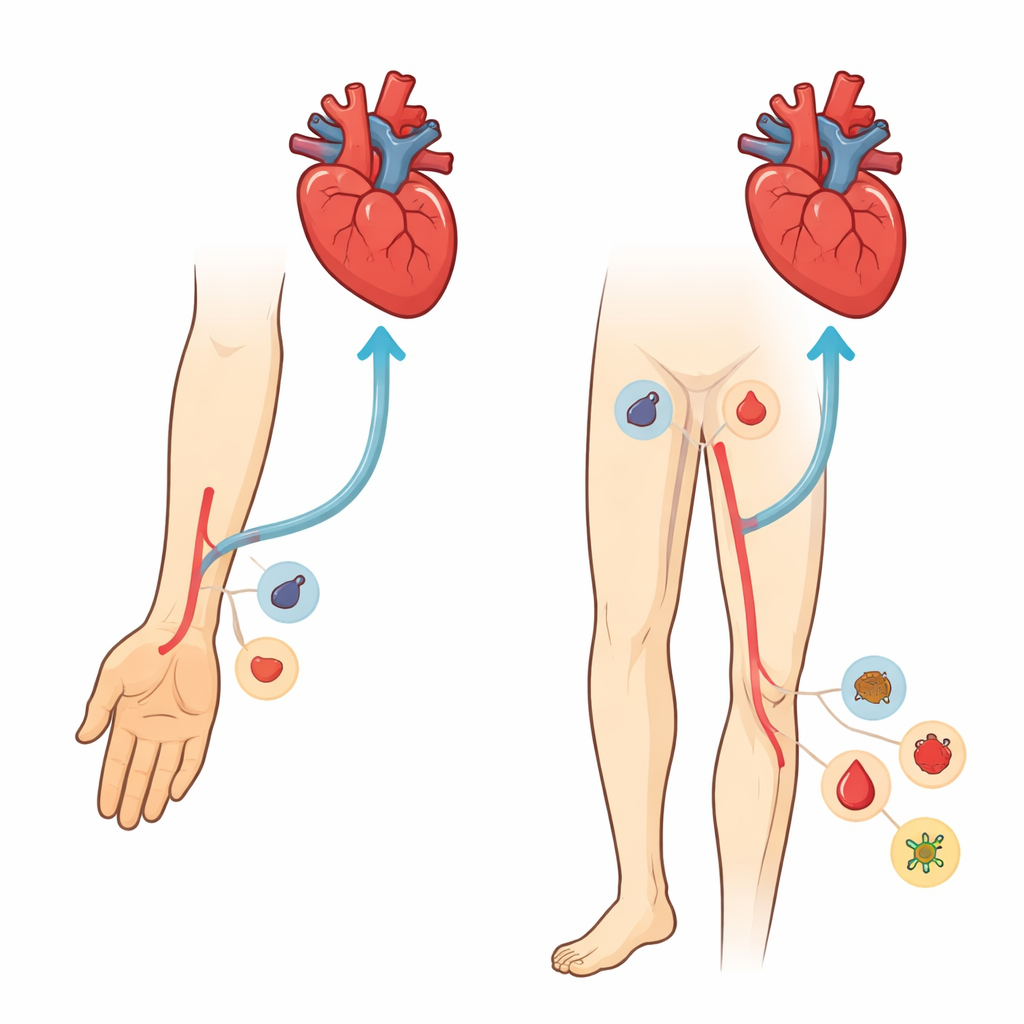
Two Roads to the Heart
The review compares two main access points for procedures that open blocked heart arteries: the radial artery at the wrist and the femoral artery in the groin. Large clinical trials and pooled analyses now show that, especially in people with heart attacks and other acute coronary syndromes, going through the wrist lowers the risk of major bleeding, blood vessel damage, and even death, compared with the groin route. Overall, wrist access has vascular complication rates around or below 1%, while groin access can reach several percent. The benefit is greatest in sicker, higher‑risk patients, where even a single bleeding event can tip the balance toward heart failure, kidney injury, or death.
What Can Go Wrong at the Wrist
Although wrist access is safer overall, it is not risk‑free. During the procedure, the radial artery can go into painful spasm that makes it hard to advance the catheter; rarely, the vessel wall can tear or perforate. After the procedure, the artery can clot off (radial artery occlusion), which is usually silent but can prevent reuse of that artery for future procedures or bypass surgery. Other uncommon problems include hematomas (localized collections of blood under the skin), small false aneurysms, abnormal artery‑to‑vein connections, nerve irritation, and, in extreme cases, dangerous pressure build‑up in the forearm compartment. The article details how careful needle placement with ultrasound, use of smaller and smoother sheaths, adequate numbing and sedation, blood thinning during the case, and “patent” (non‑crushing) compression afterward dramatically reduce these complications and often allow them to be handled with simple measures instead of surgery.
Risks Unique to the Groin Route
Problems around the femoral artery tend to be less common in modern practice, mainly because the groin route is used less often, but they are often more severe when they occur. Bleeding can spread deeply into the pelvis as a retroperitoneal hematoma, sometimes without obvious bruising on the skin, and is linked to higher short‑term death rates. Large pseudoaneurysms and artery‑to‑vein fistulas can cause pain, limb swelling, or heart strain and may need clot‑forming injections, stents, or open surgery. There is also a small risk of limb‑threatening ischemia when the artery is narrowed or blocked by plaque, clots, or closure devices. The review emphasizes meticulous puncture technique guided by ultrasound and X‑ray landmarks, appropriate sheath size, and rapid recognition of falling blood pressure or leg symptoms so that bleeding can be stopped with balloons, covered stents, or surgery before permanent harm occurs.
Shared Hazards: Brain, Kidneys, and Radiation
Some dangers do not depend much on where the catheter enters. Stroke during or soon after a coronary procedure is rare but devastating, usually caused by small clots or fragments of plaque that travel to the brain. The risk rises with older age, prior stroke, complex devices, and more catheter exchanges. Kidney injury is another major concern, driven largely by the amount of X‑ray contrast dye, low blood pressure, and bleeding. Hydration before and after the procedure, limiting contrast volume, and avoiding large blood losses all help protect the kidneys. Interestingly, trials suggest that wrist access modestly reduces kidney injury, probably because it leads to fewer major bleeds rather than using less contrast. Finally, the article notes that wrist procedures may slightly increase radiation exposure in some settings, underscoring the need for strict radiation‑safety habits.
Looking Ahead: Smarter Access Choices
The authors highlight several emerging solutions. New access sites, such as the distal radial artery near the thumb or the ulnar artery, may further cut down on wrist artery occlusion and preserve future options, though they are technically more demanding and more likely to require switching to another site mid‑procedure. Artificial intelligence tools are being developed to combine a patient’s age, kidney function, bleeding risk, and vessel anatomy to recommend the safest entry point and contrast strategy for each case. The overall message is that choosing the wrist over the groin, when possible, prevents many complications; but thoughtful patient selection, careful technique, and tailored aftercare remain essential. With better planning and smarter tools, doctors hope to make life‑saving heart interventions even safer while preserving the arteries patients may need again in the future.
Citation: Attachaipanich, T., Khawaja, M., Takahashi, E.A. et al. Percutaneous Coronary Intervention and vascular access complications: A contemporary review. npj Cardiovasc Health 3, 23 (2026). https://doi.org/10.1038/s44325-026-00125-6
Keywords: transradial access, transfemoral access, vascular complications, percutaneous coronary intervention, bleeding risk