Clear Sky Science · en
Comparison of mixed reality and computed tomography-guided preoperative hook-wire localization for pulmonary nodules in video-assisted thoracoscopic surgery: a noninferiority randomized clinical trial
Seeing Hidden Spots in the Lungs
Tiny spots in the lungs can be early signs of cancer, but they are hard to find and remove safely. Before keyhole lung surgery, doctors place a thin wire to mark each spot so it can be found during the operation. This study asks whether new mixed reality headsets can help doctors place these wires more quickly and safely than the usual method that relies on repeated CT scans.
Why Marking Lung Spots Matters
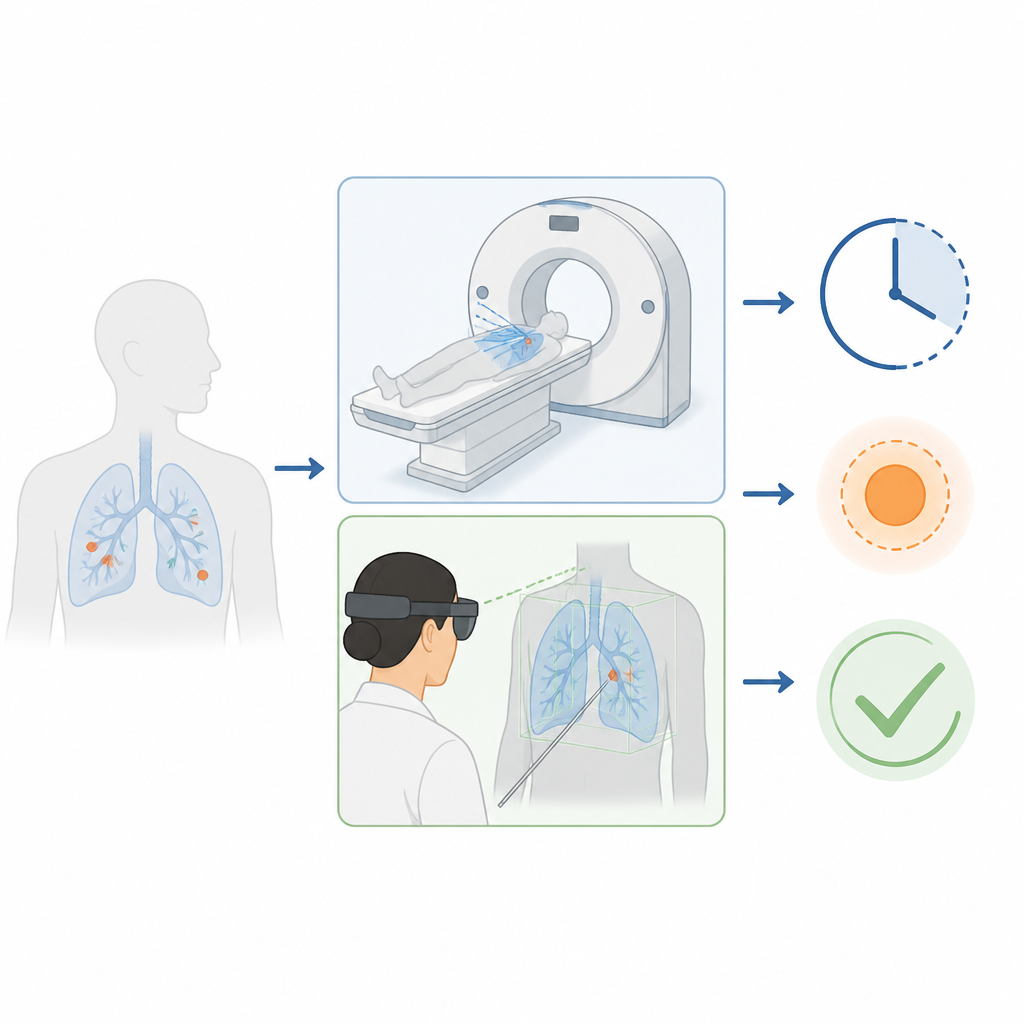
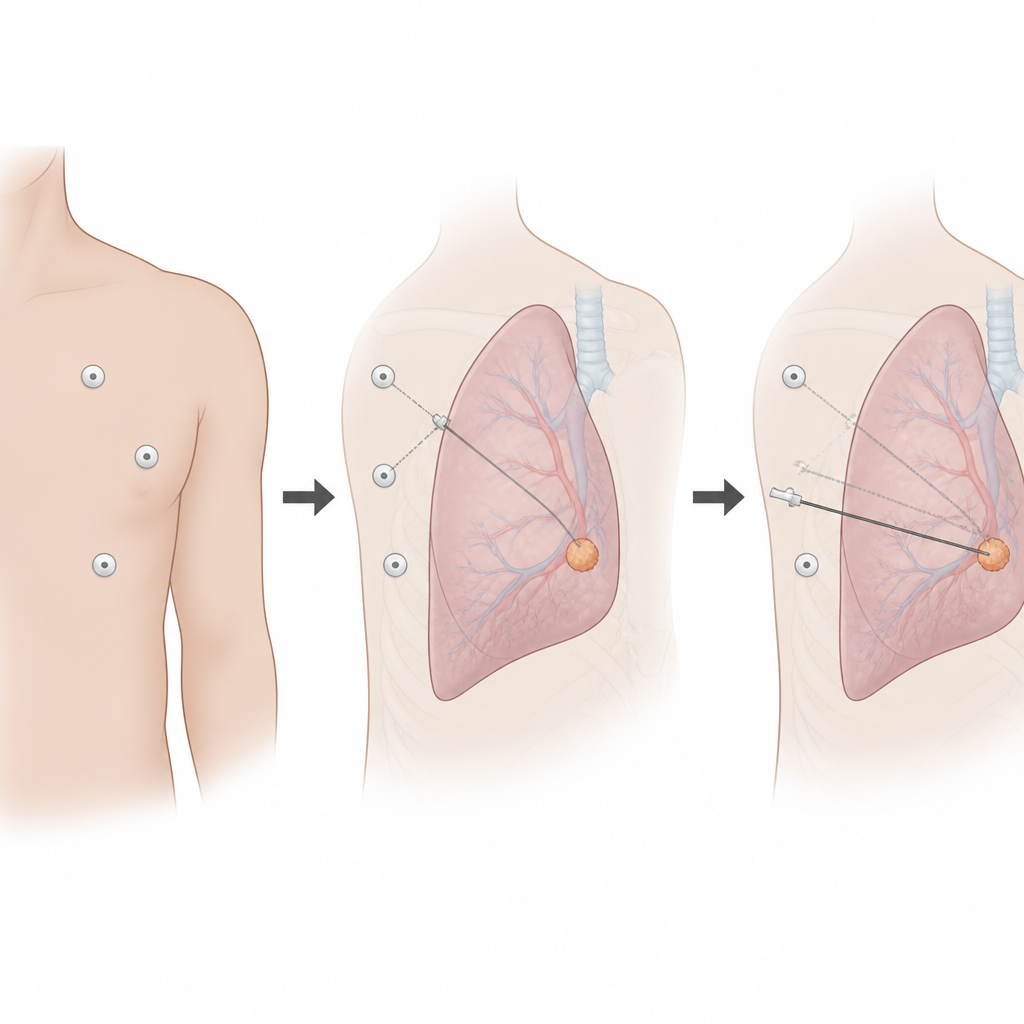
When a small lung nodule needs to be removed, surgeons often use video-assisted thoracoscopic surgery, or VATS, which uses small cuts instead of opening the chest. Because the lung is full of air and the nodules are often less than two centimeters across, they can be almost impossible to see or feel during surgery. To solve this, a radiologist places a slender hook wire through the chest wall so its tip sits next to the nodule, giving the surgeon a guide. The standard way to do this uses CT images taken over and over as the doctor slowly adjusts the wire, which costs time, exposes everyone to radiation, and can cause pain or lung collapse.
How Mixed Reality Changes the View
Mixed reality blends a computer-made image with the real world. In this trial, doctors first created a three-dimensional model of each patient’s lungs and nodules from a CT scan. They then placed three reflective markers on the patient’s chest and used cameras and a headset to match the digital model to the actual body surface. Through the headset, the doctor could see a transparent image of the lung and the nodule lined up with the real chest, along with a preplanned straight path for the hook wire. This let the doctor guide the needle by sight, almost as if they could see through the skin, and required only a checkup CT at the end to confirm the wire position.
Testing the Two Methods Head to Head
The researchers ran a randomized clinical trial with 90 adults who had single small lung nodules and were scheduled for VATS. Half were assigned to the standard CT-guided wire placement and half to the mixed reality approach. The main measure was how close the final hook wire ended up to the nodule. Other measures included how long the procedure took, how many times the needle had to be inserted, how much radiation was used, and whether problems such as lung collapse or bleeding occurred. The study was designed as a noninferiority trial, meaning the new method only needed to be at least as accurate and safe as the usual CT guidance, not necessarily better.
What the Study Found in Practice
The mixed reality method did more than just match CT guidance. On average, the distance between the wire and the edge of the nodule was slightly smaller with mixed reality than with standard CT guidance, especially in the up and down direction inside the chest. This met the trial’s threshold for showing that mixed reality was not inferior. At the same time, the new method was much faster, cutting procedure time from about eleven minutes to about four minutes. Patients in the mixed reality group almost always needed only one needle insertion, while those in the CT group commonly needed more than two. Because the headset method relied on a single planning scan and a final check, patients received fewer CT scans and about half the radiation dose. Rates of lung collapse, bleeding, or wire dislodgement were a bit lower with mixed reality but not clearly different in a statistical sense, and surgery results such as blood loss and hospital stay were similar in both groups.
What This Means for Future Care
For patients, the message is that mixed reality can help doctors place lung markers as accurately and safely as the current CT-based approach while using less time and radiation. The technique requires added preparation and special equipment, but it may free up busy scanners, reduce needle passes, and smooth the path to surgery. The authors conclude that mixed reality is a practical alternative for guiding wire placement before keyhole lung surgery and may improve comfort and workflow. Larger studies in different hospitals, and careful cost checks, will be needed before such headsets become a routine part of preparing for lung nodule surgery.
Citation: Qi, W., Zhou, J. & Xin, N. Comparison of mixed reality and computed tomography-guided preoperative hook-wire localization for pulmonary nodules in video-assisted thoracoscopic surgery: a noninferiority randomized clinical trial. Sci Rep 16, 15690 (2026). https://doi.org/10.1038/s41598-026-47315-x
Keywords: mixed reality, pulmonary nodules, CT-guided localization, thoracoscopic surgery, radiation exposure