Clear Sky Science · en
Antifungal susceptibility and in vitro virulence characteristics of clinical Magnusiomyces/Saprochaete isolates: a multicenter study from Türkiye
Why hidden hospital fungi matter
In modern hospitals, many seriously ill patients survive thanks to intensive care, cancer therapy, and organ transplants—but these same treatments weaken their defenses against infection. This study looks closely at an under‑recognized group of hospital fungi, Magnusiomyces (formerly called Saprochaete), that can cause severe disease in people with fragile immune systems. By tracking how often these fungi appear, how dangerous they are, and which medicines still work, the researchers aim to give doctors better tools to protect some of the sickest patients.
Uncommon germs in vulnerable patients
Invasive fungal infections kill an estimated 1.5 million people worldwide each year, and most attention goes to well‑known culprits like Candida and Aspergillus. Magnusiomyces species are rarer, yeast‑like fungi that live in soil, water, plants, and sometimes on human skin and mucous membranes. In healthy people they rarely cause trouble, but in patients with blood cancers, organ transplants, or long stays in intensive care units, they can move from harmless passengers to life‑threatening invaders of the bloodstream and organs. Because they resemble other fungi under the microscope and resist some standard drugs, they are easily misidentified or overlooked.
Gathering clues from hospitals across Türkiye
The team collected 133 Magnusiomyces isolates from 18 hospitals in 10 Turkish cities, spanning 2010–2024. Most came from older adults—especially men—and were found in urine, sputum, endotracheal aspirates, and blood, reflecting both localized and potentially widespread infection. A striking spike in cases occurred in 2022, a time when hospitals were still under heavy strain after the COVID‑19 pandemic, with crowded intensive care units, prolonged antibiotic use, and frequent use of invasive devices such as catheters and ventilators. These conditions are ideal for opportunistic fungi to take hold and spread.
Pinpointing the exact fungus
Correctly naming these fungi is critical because closely related species can behave differently and respond differently to treatment. The researchers re‑identified all isolates using a rapid protein fingerprinting tool called MALDI‑TOF MS and confirmed the results with DNA sequencing of two genetic regions. About four out of five isolates were Magnusiomyces capitatus and one out of five were Magnusiomyces clavatus. The two methods agreed in 99.2% of cases, showing that modern mass‑spectrometry, backed up by genetic testing when needed, can reliably distinguish these look‑alike species. A genetic family tree of the isolates showed a scattered pattern rather than tight clusters, suggesting that infections arose independently in many hospitals rather than from a single nationwide outbreak.
Which antifungal drugs still work?
To guide therapy, the team measured how much of each drug was needed to halt fungal growth in the lab. There are no official breakpoints for Magnusiomyces, so they compared drug strengths by their minimum inhibitory concentrations. Across both species, voriconazole, amphotericin B, and posaconazole required the lowest concentrations, indicating relatively good activity. Itraconazole and flucytosine were less consistent, and fluconazole—the most commonly used yeast drug worldwide—performed the worst, with very wide and mostly high concentration ranges. This pattern reinforces earlier case reports showing that standard fluconazole‑based treatment can easily fail against these fungi, and that doctors should instead consider voriconazole or amphotericin B when Magnusiomyces is suspected.
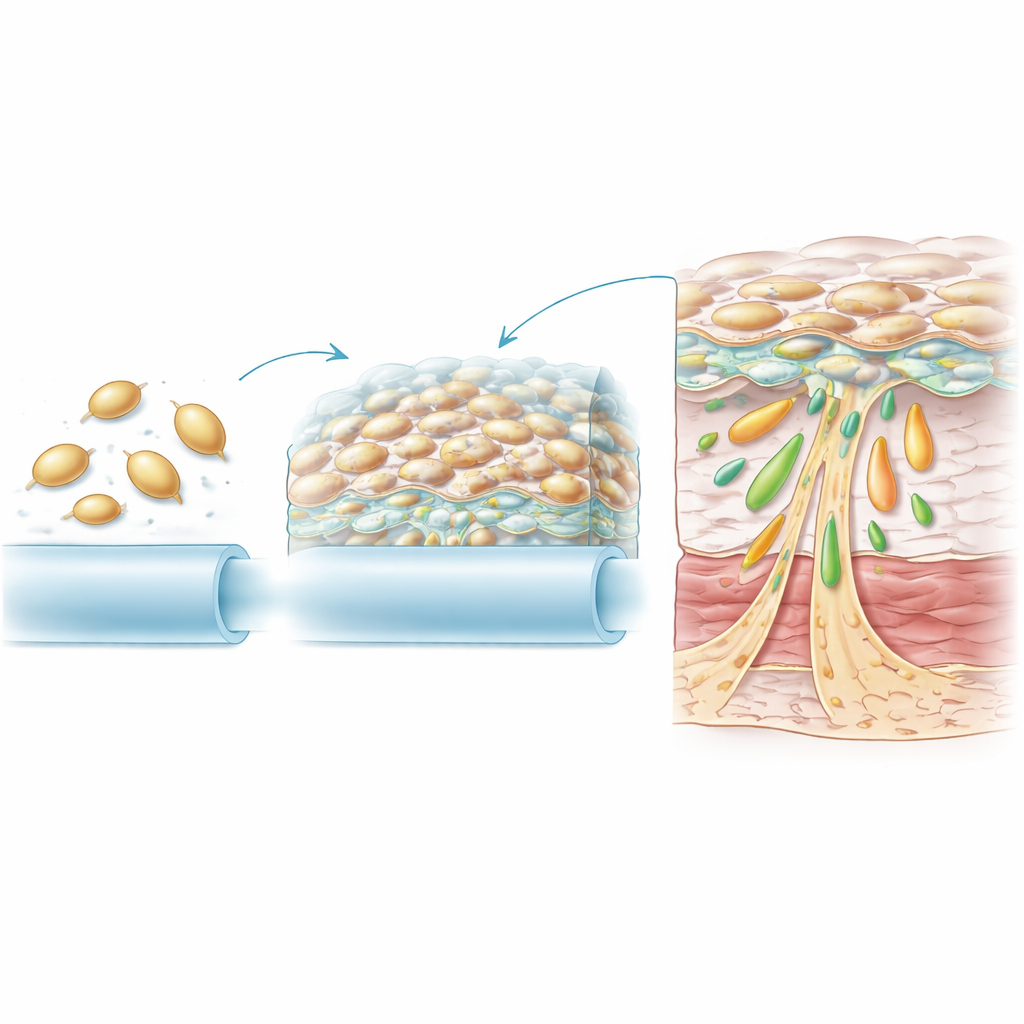
How these fungi cling, persist, and damage tissue
Drug resistance is only part of the story. The researchers also tested several traits that help fungi cause disease. Almost all isolates were strong biofilm producers, meaning they could form dense, slimy communities on plastic and other surfaces that shield them from drugs and the immune system. Magnusiomyces capitatus was especially powerful in this regard, which fits with its frequent recovery from indwelling devices such as catheters. Both species also produced enzymes that break down fats and proteins in body tissues. Magnusiomyces clavatus showed particularly high levels of caseinase and esterase activity, suggesting a strong ability to invade and damage deep tissues, while some isolates of both species secreted other destructive enzymes and showed blood‑cell‑damaging activity.
What this means for patients and care teams
For a lay reader, the key message is that a little‑known set of hospital fungi is quietly gaining ground among the most vulnerable patients. This large multicenter study from Türkiye shows that Magnusiomyces species are widespread, difficult to eradicate because of strong biofilm formation and tissue‑degrading enzymes, and not reliably controlled by standard fluconazole therapy. Fast, species‑level identification with modern laboratory tools, combined with early use of better‑performing drugs like voriconazole or amphotericin B, may improve outcomes. As hospitals continue to care for growing numbers of immunocompromised people, understanding and recognizing these rare fungi becomes an important part of keeping high‑risk patients safe.
Citation: Ozturk, A., Aydin, M., Sahin, E.A. et al. Antifungal susceptibility and in vitro virulence characteristics of clinical Magnusiomyces/Saprochaete isolates: a multicenter study from Türkiye. Sci Rep 16, 13549 (2026). https://doi.org/10.1038/s41598-026-42967-1
Keywords: invasive fungal infection, Magnusiomyces, immunocompromised patients, antifungal resistance, biofilm