Clear Sky Science · en
Measures to monitor the implementation of Essential Health Benefit Packages at a national scale
Why this matters for everyday health
When people think about healthcare, they often ask, “Is there a clinic nearby?” But being close to a clinic doesn’t help if it lacks medicines, tests, or trained staff. This study looks at Malawi, a low-income country in southern Africa, to ask a simple but vital question: how many people actually live within reach of clinics and hospitals that are truly prepared to deliver essential care—from vaccines and childbirth services to heart disease treatment and surgery?
Looking beyond distance to real access
Many governments now define “essential health benefit packages,” lists of services that everyone should be able to receive as part of universal health coverage. Yet most countries struggle to track who is actually covered. Traditional household surveys are excellent for a few common services such as childhood vaccines, but they rarely cover the full range of care people need, and they ignore whether facilities are stocked and staffed. The researchers behind this study used a different strategy: they combined a nationwide survey of health facilities in Malawi with detailed population maps to estimate who lives close to facilities that are ready to deliver specific services.
Checking if clinics are truly ready
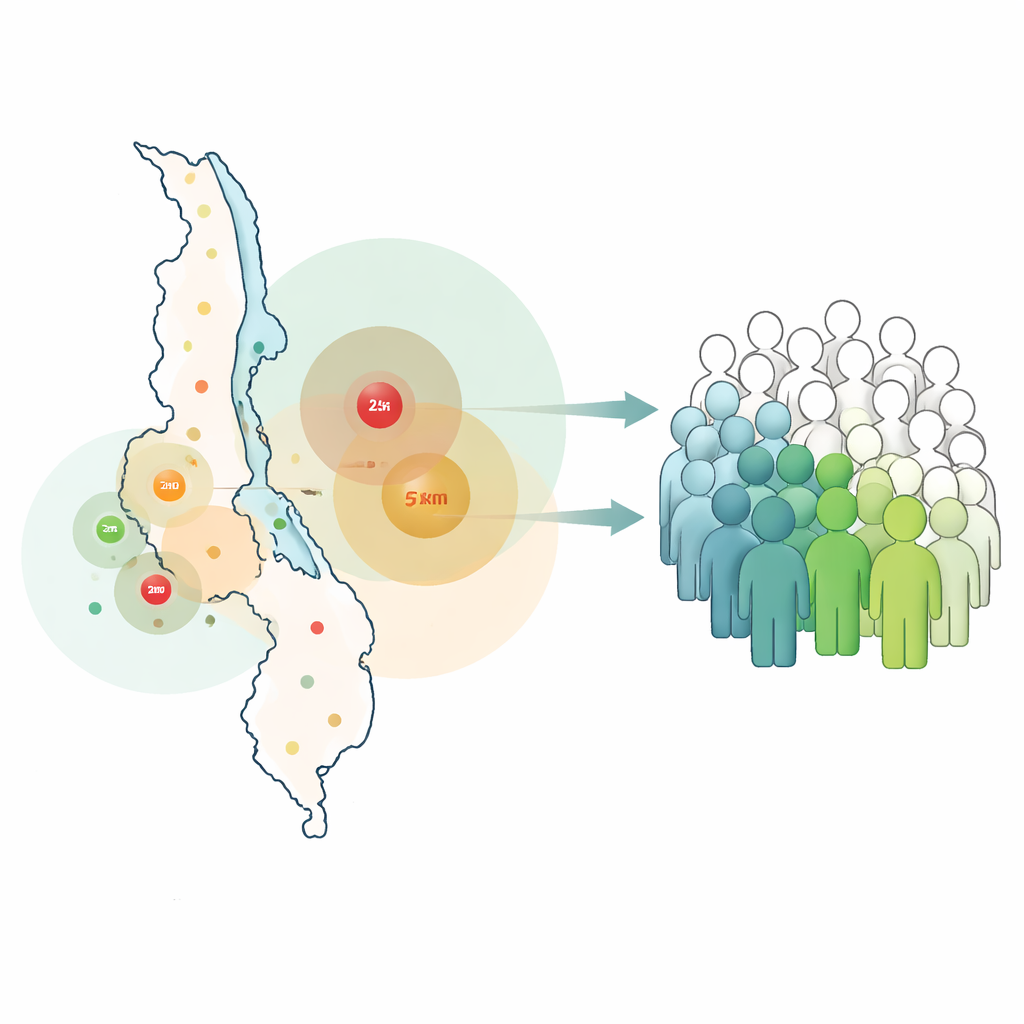
The team began with a global list of cost‑effective, high‑priority health interventions and matched 280 of them to questions asked in Malawi’s 2019 Harmonized Health Facility Assessment. For 129 services, they could build “readiness” checklists that included basics like infrastructure, diagnostic tests, medicines, and trained health workers. A facility was counted as ready for a service only if all minimum ingredients were present. They then used map‑based analysis to draw catchment circles—5 kilometers around primary care facilities and 25 kilometers around higher‑level hospitals—and overlaid these with fine‑grained population data to see what share of Malawians lived within reach of a ready facility.
Where Malawi is doing well
The results show clear successes in areas that have long been backed by national policy and international donors. Facilities were generally well prepared for childhood vaccinations, HIV treatment, and malaria care. For example, most clinics had the basic tools and medicines to treat uncomplicated malaria, and more than half of the population lived within 5 kilometers of a facility ready to deliver that care. Similar patterns appeared for first‑line HIV treatment and some sexually transmitted infection services, where both readiness and population coverage were relatively high across the country.
The quiet shortage in chronic and surgical care
In sharp contrast, services for long‑lasting conditions and more complex treatments lagged badly. Very few facilities were ready to provide ongoing care for chronic asthma or chronic obstructive lung disease, and only a small fraction of Malawians lived near facilities prepared to manage these conditions. Readiness for heart disease care was also strikingly low, with many district hospitals lacking key tests, drugs, or staff, and only a modest share of the population within range of hospitals able to treat heart attacks or acute heart failure. Surgical care showed similar gaps, with only a minority of higher‑level hospitals equipped to perform essential operations. Maps by district revealed large geographic differences: some areas had relatively good coverage for services like HIV treatment or family planning, while coverage for diabetes and chronic lung disease was poor almost everywhere.
Turning data into better planning
Beyond the headline numbers, the method itself is a key contribution. By tracing “readiness cascades” for each service, the authors could pinpoint which missing input—such as a specific instrument, a lab test, or a medicine—caused the largest drop in capacity. They also showed that many “not applicable” entries in the survey effectively signaled that certain services simply are not offered at particular types of facilities, especially for chronic and advanced care. The approach can be repeated over time and adapted to other countries using similar facility surveys, giving health ministries a practical way to align their benefit packages with what the system can actually deliver, and to decide where investments in supplies, equipment, or staff will close the biggest gaps.
What this means for patients and policymakers
In everyday terms, the study shows that Malawi has made real strides in services that have been priorities for decades, like childhood vaccination, HIV, and malaria—but that people with chronic illnesses or surgical needs often remain far from ready care. The new “input‑adjusted coverage” measure does not track who actually uses services or how good the care is, but it does answer a crucial question: is there a properly equipped facility close enough to reach? By combining readiness checks with maps of where people live, this work offers a clearer, more realistic picture of who is truly covered and where the health system needs to grow next.
Citation: Ahmed, S., Sun, J., Cao, Y. et al. Measures to monitor the implementation of Essential Health Benefit Packages at a national scale. npj Health Syst. 3, 27 (2026). https://doi.org/10.1038/s44401-026-00081-4
Keywords: universal health coverage, health facility readiness, Malawi health system, geospatial health access, essential health services