Clear Sky Science · en
The performance of FIT-based colorectal cancer screening: results from a population-based program
Why this matters for everyday health
Colorectal cancer is one of the world’s deadliest cancers, yet it is often curable when found early. The gold-standard test, colonoscopy, can spot and remove precancerous growths, but it is expensive, time-consuming, and many people are reluctant to undergo it. This study from northern China asks a practical question with global relevance: can we use a simple home stool test to decide who most urgently needs a colonoscopy, saving money and effort while still catching cancers early?
A simple home test to guide a big decision
The research focused on the faecal immunochemical test, or FIT, a kit that people can use at home to check for tiny traces of blood in their stool. Blood can be an early warning sign of growths in the colon, including polyps and cancers. In this large public program, more than 120,000 city residents aged 45 to 74 first completed both a FIT and a short questionnaire about lifestyle and medical history. Anyone with either a positive FIT or high-risk answers on the questionnaire was offered a free colonoscopy in a hospital. This two-step approach mirrors real-world constraints: colonoscopy resources are limited, so health systems must decide who most needs this more invasive test.
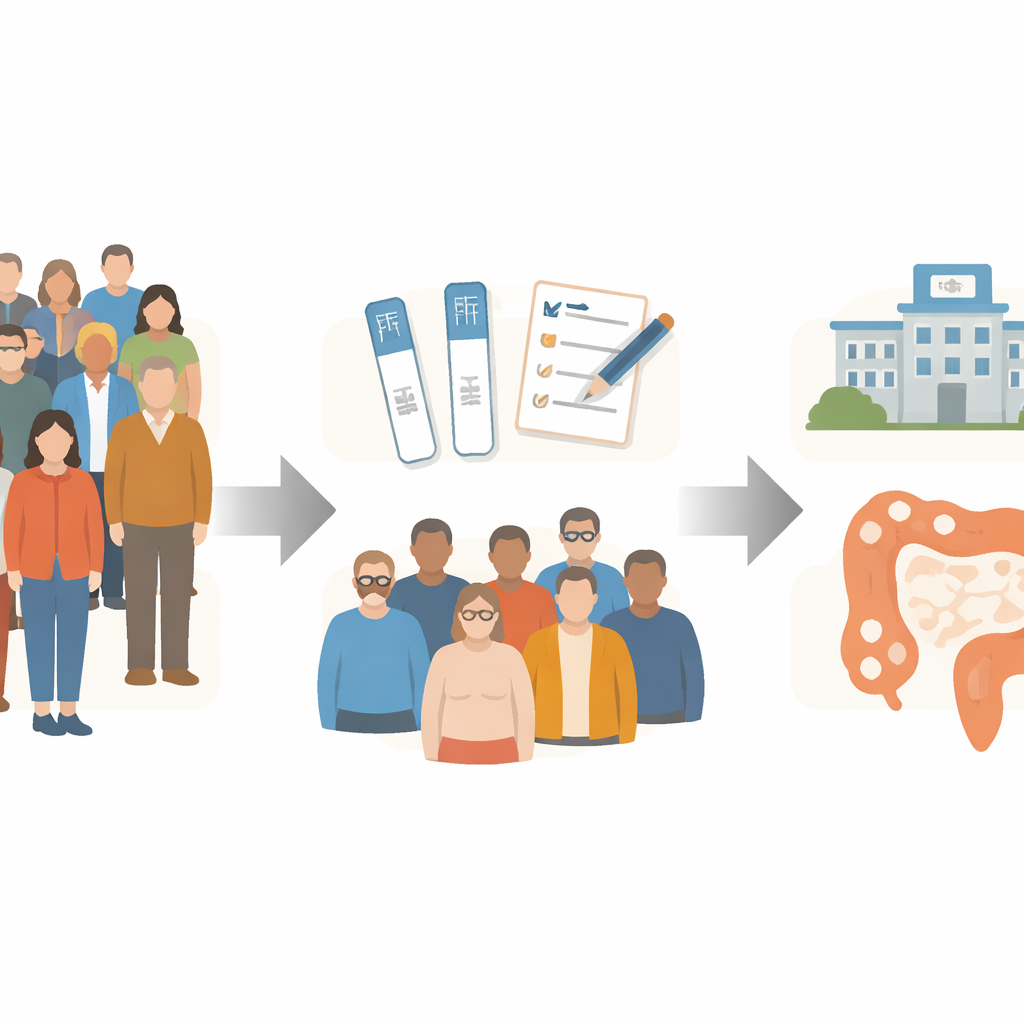
Who showed up and what doctors found
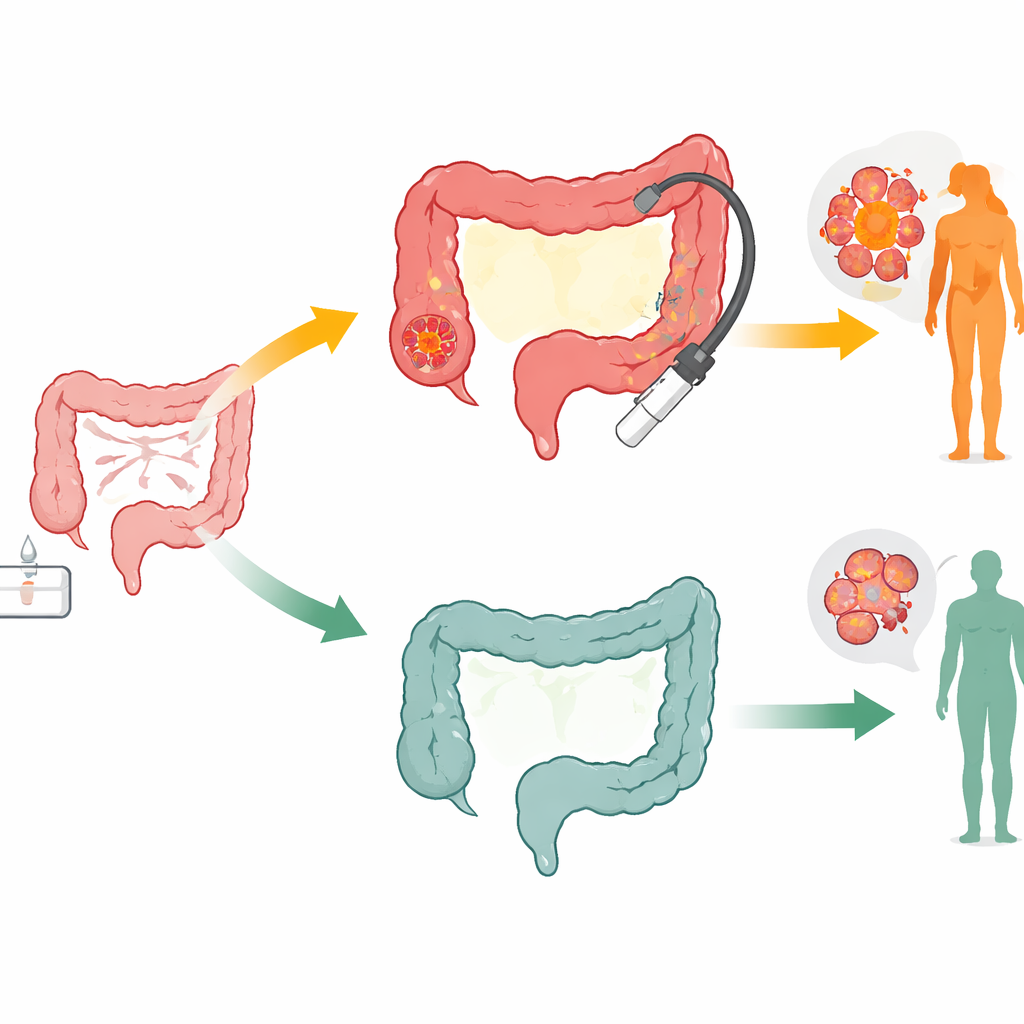
Among about 44,000 people labeled high-risk, roughly one in six had a positive FIT result. These FIT-positive individuals were more likely to go on to colonoscopy than those who were flagged only by the questionnaire—about one in three versus one in six. Over the course of the program, colonoscopies uncovered 44 colorectal cancers and more than 2,300 precancerous polyps, including 601 advanced adenomas, which are especially likely to turn into cancer. Across all age groups and in both men and women, people with a positive FIT had higher rates of advanced growths than those with a negative FIT but risky questionnaire answers. In other words, the FIT signal was strongly linked to the truly dangerous findings doctors care about most.
Costs, value, and catching cancer early
The researchers then asked how much it actually cost the health system to find each serious lesion. When they looked at the entire screening effort, finding one cancer cost about US$22,000, and finding one advanced growth cost about US$1,500. But when they broke this down by FIT status, a striking pattern emerged. For people with a positive FIT, the cost to detect a single cancer was about 80% lower than for FIT-negative, questionnaire-positive participants. The savings were more than 50% for advanced and nonadvanced polyps. Because more FIT-positive people accepted colonoscopy and more of them had important findings, each colonoscopy in this group delivered more benefit per dollar spent.
What happened over time
Participants were followed for a little over two years. During this period, 292 people developed colorectal cancer. Cancer was more likely to occur in those who had tested FIT-positive, confirming that a positive stool test signals a higher underlying risk. Crucially, however, the FIT-positive group also had a much larger share of early-stage cancers: 40% of cancers in this group were stage I, compared with only 15% in those who were FIT-negative but high-risk by questionnaire. Earlier-stage cancers are typically easier to treat and carry a better outlook. Overall deaths were lowest among people who were screened, suggesting that taking part in the program was linked to broader health benefits, although the follow-up was still too short to show clear differences in deaths specifically from colorectal cancer.
Smarter screening through combined information
Beyond simple test results, the team evaluated several risk scoring tools that combine age, sex, family history, weight, smoking, and other factors. They compared these scores alone, FIT alone, and versions that combined both. Models that blended FIT status with risk factors identified many more cancers than either method on its own, with only a modest loss in specificity. This suggests that future programs could target colonoscopy even more precisely by layering a quick questionnaire on top of the stool test, rather than relying on a single signal.
What this means for patients and health planners
For laypeople, the takeaway is straightforward: a simple at-home stool test can serve as a powerful gatekeeper, identifying who most urgently needs colonoscopy and increasing the chances that any cancer found is at an early, more curable stage. For health systems, the study shows that combining FIT with a short risk questionnaire makes large-scale screening more affordable and efficient, especially where colonoscopy capacity is limited. While longer follow-up is needed to fully measure the impact on cancer deaths, the evidence supports FIT-based strategies as a practical backbone for national colorectal cancer screening programs.
Citation: Shi, J., Li, Z., Liang, D. et al. The performance of FIT-based colorectal cancer screening: results from a population-based program. Sci Rep 16, 13902 (2026). https://doi.org/10.1038/s41598-026-48840-5
Keywords: colorectal cancer screening, fecal immunochemical test, colonoscopy, early cancer detection, public health programs