Clear Sky Science · en
Paraspinal muscle fatty infiltration is associated with nonunion and cage subsidence after anterolateral lumbar interbody fusion: a level-specific analysis
Why the Muscles Around Your Spine Matter
Lower back fusion surgery is often the last resort for people with stubborn back pain or leg pain that will not improve with rest, therapy, or injections. Surgeons place a small spacer, or cage, between two back bones to help them grow together into one solid piece. But in some patients the bones fail to unite, or the cage slowly sinks into the bone, leading to persistent pain and possible repeat surgery. This study asks a simple but important question: does the condition of the deep back muscles that hug the spine help determine whether a fusion will succeed or fail?
The Problem of Bone Healing After Back Surgery
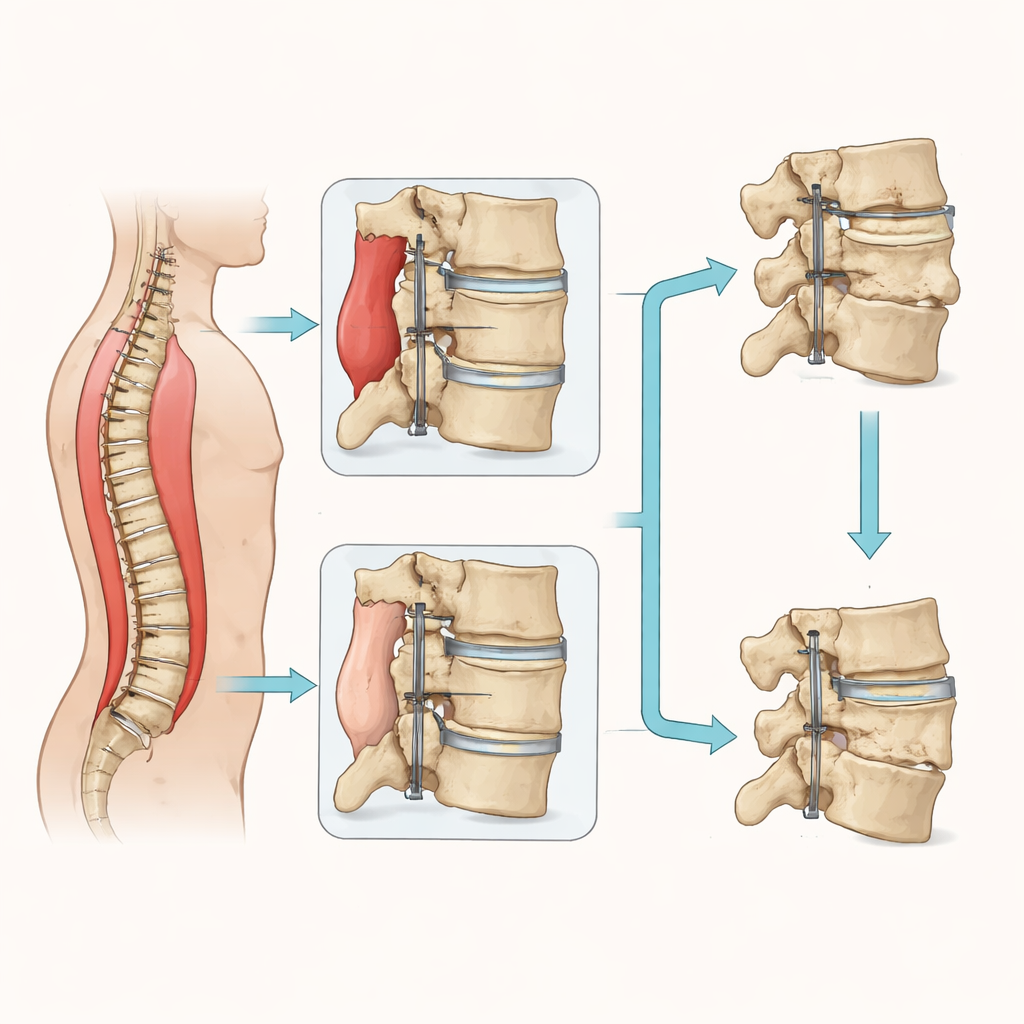
In anterolateral lumbar interbody fusion, surgeons reach the spine from the front or side, slide out the damaged disc, and insert a cage filled with bone graft between the vertebrae. Metal screws and rods at the back add support. Ideally, new bone grows through and around the cage, locking the bones together. When this does not happen, called nonunion, patients can remain in pain and the hardware may loosen. Another complication, cage subsidence, occurs when the cage slowly presses down into the soft underlying bone, changing alignment and increasing the risk of nonunion. Doctors know that smoking, extra body weight, and poor bone quality can all raise these risks, but the role of the surrounding muscles has been less clear.
Fat Versus Muscle Around the Spine
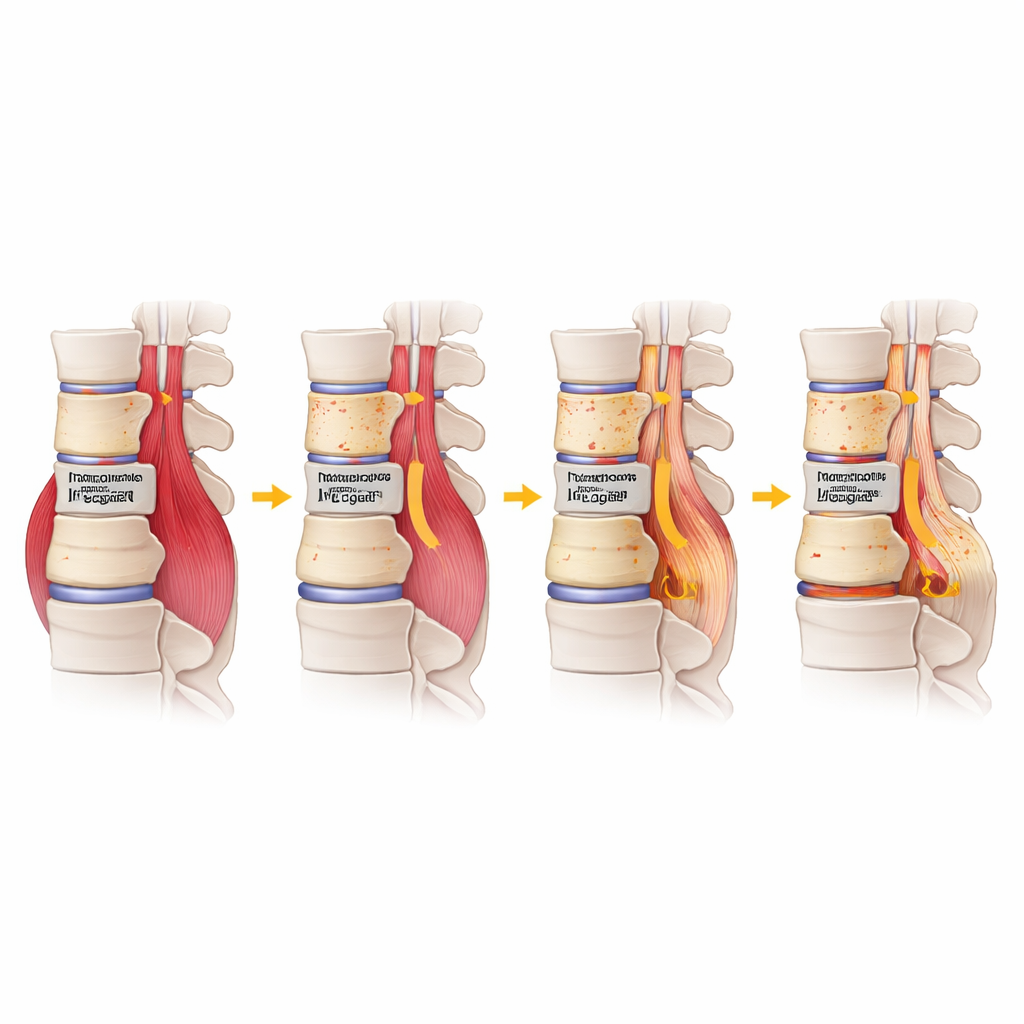
The paraspinal muscles run up and down along either side of the spine and help keep the trunk upright and stable. With age, inactivity, or long-standing back problems, these muscles can shrink and be partly replaced by fat. Using preoperative MRI scans from 127 patients who had single-level fusion from the front or side, the researchers measured both the size of these muscles and how much fat had crept into them, just above and just below the level being fused. Muscle size was expressed relative to the size of the nearby vertebral body, while muscle quality was captured by the amount of fatty infiltration, a way of saying how much of the muscle space was actually fat instead of working muscle.
Linking Muscle Quality to Surgical Outcomes
Two years after surgery, the team checked X‑rays to see which patients had solid fusion and which had nonunion, and whether the cage had subsided by at least two millimeters. About one in six patients showed nonunion and one in five had cage subsidence. When the researchers compared those with good and poor results, traditional factors such as body mass index and smoking were more common in the failure groups, but the clearest pattern involved muscle quality. Patients whose deep back muscles below the fused segment were more heavily infiltrated with fat were significantly more likely to have nonunion and, in many cases, cage subsidence as well. A critical threshold emerged: when fatty infiltration below the fusion exceeded roughly 56 percent, the chance of the bones not uniting rose sharply.
Where in the Spine the Effect Is Strongest
The lumbar spine is not uniform from top to bottom. The junction between the lowest lumbar vertebra and the sacrum bears different loads than the upper levels. To account for this, the researchers separated patients whose surgery involved the upper lumbar levels (L1–L4) from those whose fusion was at L5–S1. In the upper levels, high fat content in the muscles beneath the fused segment remained a strong predictor of both nonunion and cage sinking, even after adjusting for age and smoking. In contrast, at the L5–S1 level, body weight appeared to play a larger role than muscle quality, likely because this junction experiences especially high compression forces from the entire upper body.
What This Means for Patients and Surgeons
Together, these findings suggest that how healthy and "lean" the deep back muscles are—rather than simply how big they look—matters for the success of front or side lumbar fusion, particularly in the upper part of the lower back. Muscles riddled with fat may provide less active support and fewer biological signals needed for robust bone healing, making it harder for a cage to stay well seated and for strong bone bridges to form. For patients, this work supports the idea that improving muscle quality through targeted exercise or conditioning before surgery could be just as important as quitting smoking or managing weight. For surgeons, routinely checking paraspinal muscle fatty change on preoperative MRI may help in selecting patients, counseling them about risk, and tailoring surgical techniques to give each fusion the best chance to succeed.
Citation: Liu, CS., Tung, KK., Chen, KH. et al. Paraspinal muscle fatty infiltration is associated with nonunion and cage subsidence after anterolateral lumbar interbody fusion: a level-specific analysis. Sci Rep 16, 14544 (2026). https://doi.org/10.1038/s41598-026-44810-z
Keywords: lumbar fusion, paraspinal muscles, muscle fat infiltration, cage subsidence, spine surgery outcomes