Clear Sky Science · en
Evaluating the efficacy of smoke management technologies in laparoscopic sleeve gastrectomy: insights from a prospective, single-centre comparative study
Why Clean Air in the Operating Room Matters
Whenever surgeons use electric scalpels or ultrasonic cutters, they create a fine smoke inside the body. This smoke can carry chemicals, tiny particles, and even living cells or viruses, potentially exposing both patients and operating-room staff to unseen risks. In keyhole procedures such as weight-loss surgery, that smoke collects in the gas used to inflate the abdomen and must be cleared safely. This study asks a practical question with big implications for safety and the environment: which of today’s smoke-clearing systems works best while using the least medical carbon dioxide (CO2)? 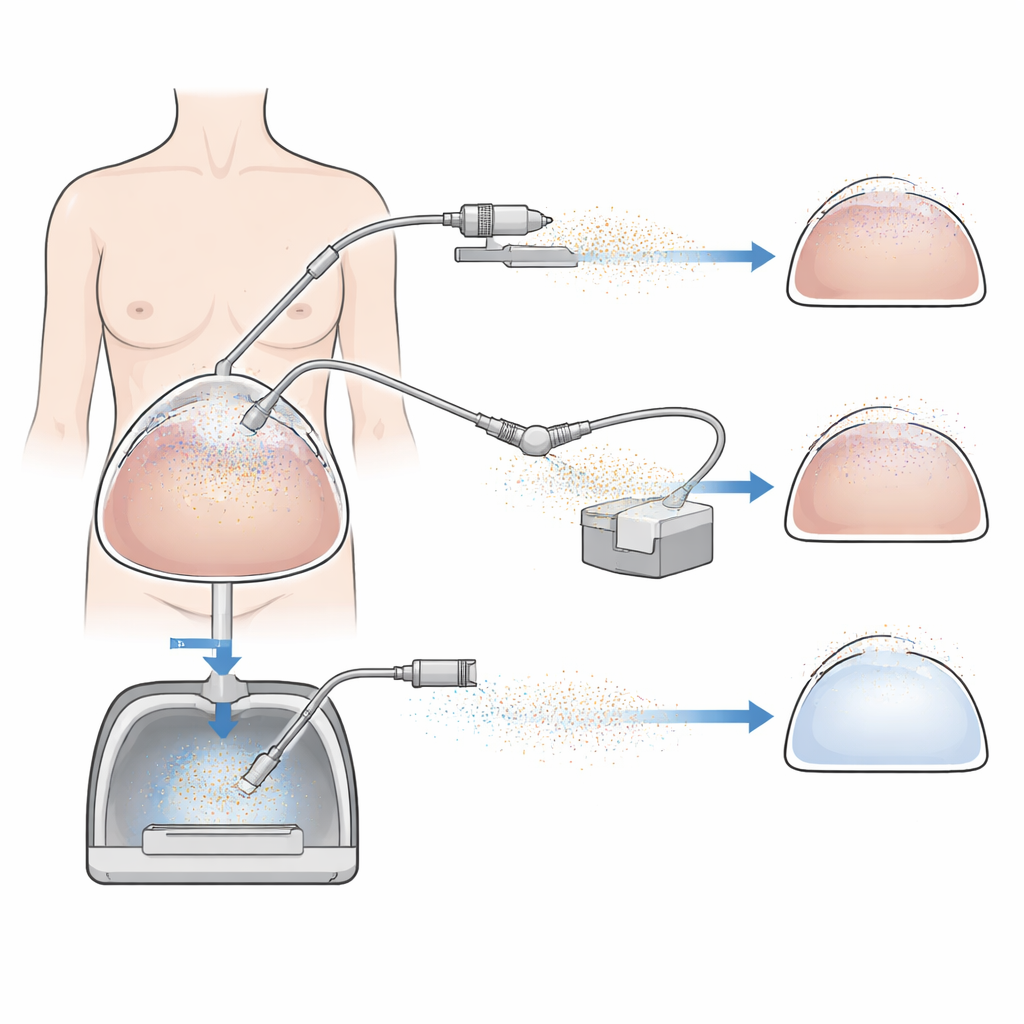
How Keyhole Weight-Loss Surgery Creates Hidden Smoke
Modern minimally invasive surgery uses high-energy devices that cut and seal tissue quickly, shortening operations and speeding recovery. But every burst of energy vaporizes a little tissue and fluid, filling the abdomen with microscopic debris. In laparoscopic sleeve gastrectomy — a common bariatric operation in which surgeons remove most of the stomach through small incisions — this smoke collects in the CO2-filled space around the organs. Traditionally, teams either vent that gas into the room or filter it, but until recently there has been little real-world data comparing how different systems perform in human patients.
Three Ways to Clear the Air
The researchers tested three technologies during sleeve gastrectomy in 15 patients at a single hospital, with each group of five patients assigned to one method. Continuous passive filtration let smoke drift out through a filter without extra suction. Continuous active filtration used a powerful device that both pumped CO2 into the abdomen and actively sucked smoky gas out through filters. The third approach, electrostatic precipitation, did something different: a small electrode charged the particles so that they stuck to the inner surfaces of the abdomen instead of floating freely in the gas. Throughout surgery, the team used sensitive particle counters to measure how quickly smoke levels fell after bursts from the cutting device, and they also tracked CO2 use, pressure stability in the abdomen, and how clearly the surgeons could see. 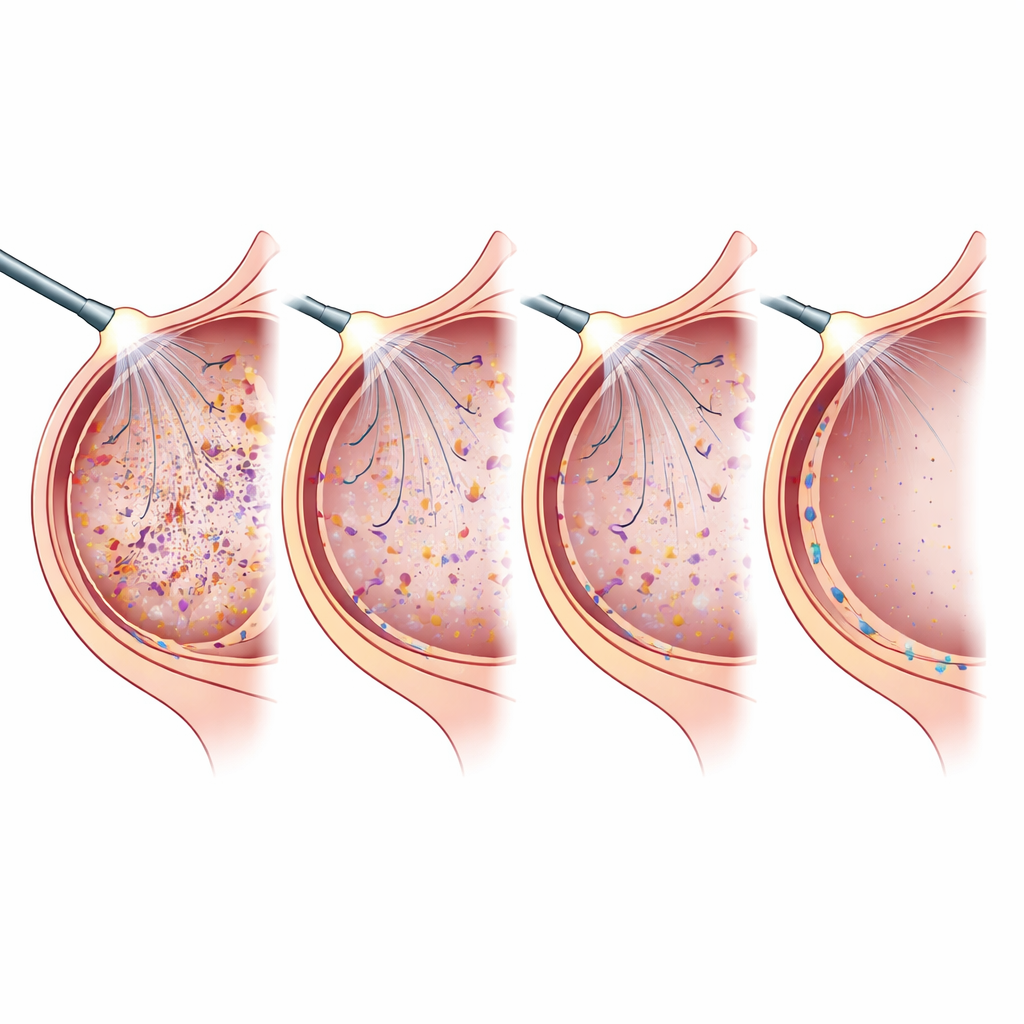
What the Measurements Revealed
To compare systems, the scientists focused on the “half-life” of smoke — how long it took for the particle concentration to drop by half after a burst. Shorter times mean faster clearing. Electrostatic precipitation was clearly the standout, halving smoke levels in about seven seconds, while the two filter-based systems took around 18 to 21 seconds. All three approaches kept the pressure in the abdomen reasonably steady and provided visibility rated as good to excellent by the surgical team. But there was a striking difference in gas consumption: the active filtration system used the most CO2 overall, the passive filter used a moderate amount, and electrostatic precipitation used only about one-third as much as the passive method and less than one-fifth as much as active filtration.
Health, Environment, and Practical Trade-Offs
Because electrostatic precipitation does not depend on constantly flushing gas through filters, it appears to release far fewer smoke particles into the operating room via leaks around the instruments. The authors estimate that if hospitals worldwide replaced evacuation-based systems with electrostatic ones for laparoscopic surgery, annual savings in medical CO2 could reach thousands of tons, with additional indirect savings from avoided industrial CO2 emissions. There were minor downsides: the lower gas flow with electrostatic systems meant the camera lens fogged a bit more at the very start of surgery, and the electrode needs to be positioned carefully to remain close enough to the surgical field. Still, these issues did not meaningfully affect operating time or overall visibility in this small trial.
What This Means for Patients and Staff
For patients, all three smoke-control methods supported safe and effective sleeve gastrectomy with good weight-loss results after one year. For surgeons and nurses, the choice of technology strongly influenced how much airborne debris and CO2 the system produced. This study suggests that electrostatic smoke removal can clean the surgical field faster, use far less CO2, and likely reduce the amount of potentially harmful smoke leaking into the room, all without sacrificing the clarity surgeons need. In everyday terms, it offers a way to keep the air cleaner, protect staff, and lighten the environmental footprint of common operations — all by quietly reshaping what happens in the invisible clouds inside a patient’s abdomen.
Citation: Demtröder, C.R.D., Göhler, D., Oelschlägel, K. et al. Evaluating the efficacy of smoke management technologies in laparoscopic sleeve gastrectomy: insights from a prospective, single-centre comparative study. Sci Rep 16, 9722 (2026). https://doi.org/10.1038/s41598-026-43227-y
Keywords: laparoscopic surgery, surgical smoke, electrostatic precipitation, bariatric surgery, medical CO2 use