Clear Sky Science · en
Gasless endoscopic thyroidectomy via the trans-subclavian approach versus conventional open thyroid surgery for unilateral thyroid cancer
Why surgery scars still matter
For many people treated for thyroid cancer, survival rates are excellent—but the experience of surgery can leave a lasting mark in other ways. A prominent scar across the front of the neck and lingering discomfort when swallowing can affect confidence, social interactions, and daily life. This study asks a simple question that matters to patients as much as to surgeons: can a newer, less visible surgical route to the thyroid remove cancer just as safely as the traditional open operation, while leaving people feeling better afterward? 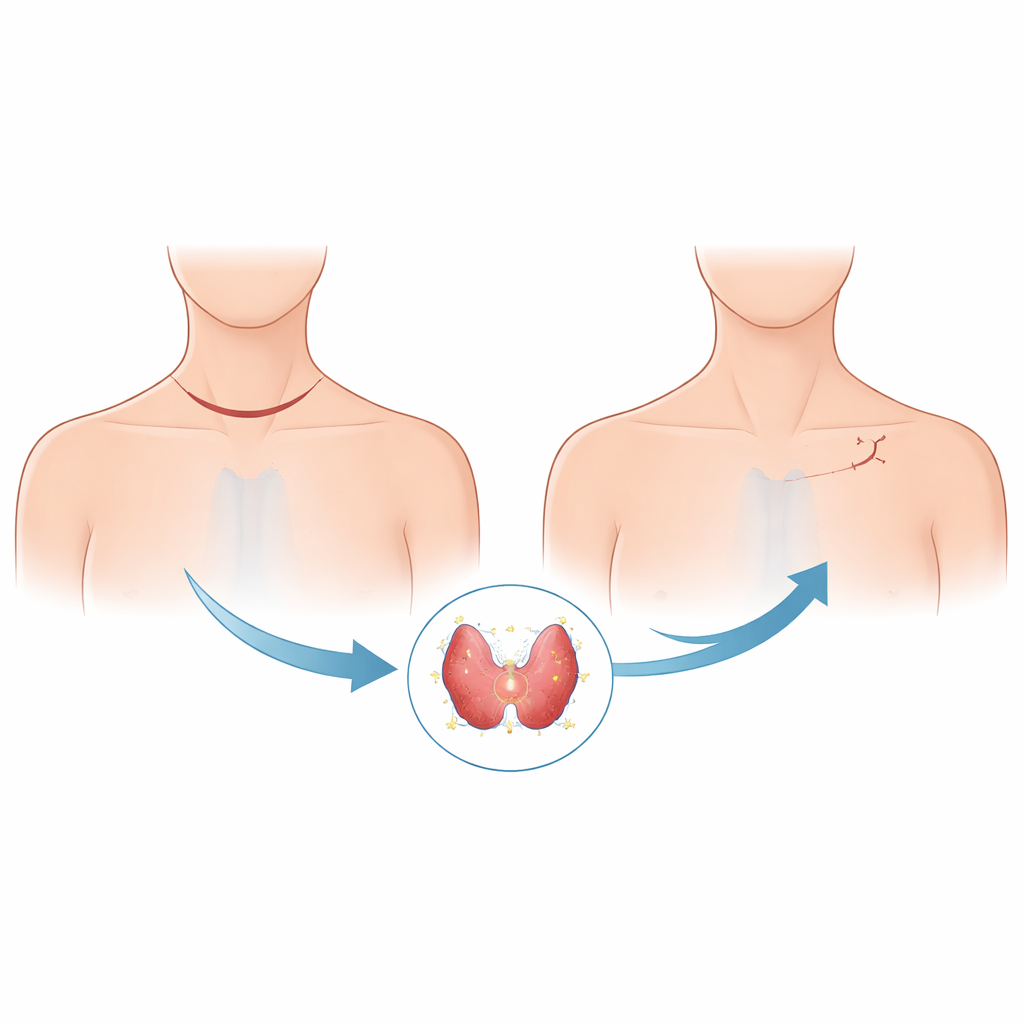
Two different paths to the same gland
The researchers focused on patients with a common type of thyroid cancer called papillary thyroid carcinoma that affected only one side of the gland. They compared the long‑established open operation, which uses a cut across the lower front of the neck, with a newer method called gasless endoscopic thyroidectomy via the trans‑subclavian approach. In this newer method, surgeons make a small incision below the collarbone, slide instruments under the muscles, and work with a camera to reach and remove the diseased half of the thyroid and nearby lymph nodes, all without filling the area with gas. Because the cut is off the neck and hidden by clothing, it promises a better cosmetic result while still allowing careful work around delicate structures such as the voice nerve and tiny parathyroid glands that control calcium balance.
Balancing the comparison
To give the two approaches a fair head‑to‑head test, the team reviewed records from 488 patients operated on at one hospital over about nine months. Not everyone is an equal candidate for every technique, so the authors used a statistical method called propensity score matching to pair 164 patients who had the open operation with 164 who had the endoscopic one but shared similar traits such as age, sex, weight, tumor size, and other health conditions. By matching people this way, differences in outcomes are more likely to reflect the surgery itself rather than who happened to receive it. They then examined not only the details of the operations and hospital stay, but also a dedicated questionnaire that measures how thyroid cancer and its treatment affect day‑to‑day quality of life.
Quality of life, scars, and time in the operating room
The results suggest that hiding the scar under the collarbone does more than just look nicer. Patients who underwent the endoscopic method reported better overall thyroid‑cancer‑related quality of life, were less bothered by their scars, and experienced slightly better swallowing comfort than those who had the classic neck incision. However, these advantages came at a cost. The endoscopic procedures took longer in the operating room and required more specialized tools, which translated into higher hospital bills and a bit more fluid draining from the surgical area right after surgery. Despite these differences, the length of hospital stay was similar between the two groups, and no patient in either group needed a second operation or suffered serious wound problems or bleeding. 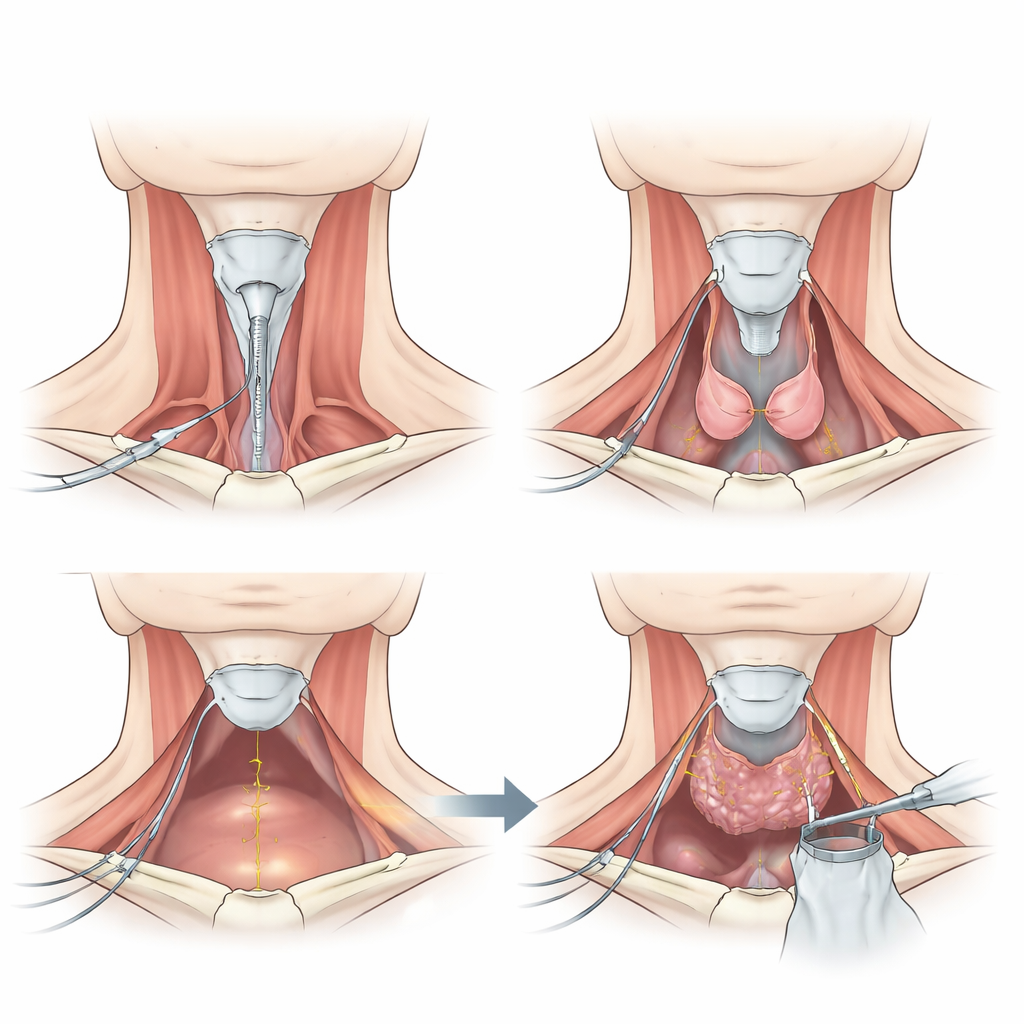
How thorough and how safe is the new route?
A key concern with any less invasive technique is whether surgeons can remove all the necessary tissue, especially lymph nodes that might harbor hidden cancer cells. In this study, surgeons retrieved fewer central neck lymph nodes on average with the endoscopic route than with the open one. Yet the number of nodes that actually contained cancer was similar in both groups, and no recurrences had appeared during the relatively short follow‑up. The use of carbon nanoparticle dye, which darkens lymph nodes and helps distinguish them from delicate parathyroid glands, likely helped surgeons working through the small endoscopic corridor. Short‑term complications were also reassuring: temporary voice weakness occurred rarely and at rates comparable to other thyroid operations, and although surgeons had to relocate parathyroid tissue more often in the endoscopic group, none of these patients showed symptoms of low calcium.
What this means for patients considering surgery
Overall, the study supports gasless endoscopic thyroidectomy through the area below the collarbone as a reliable option for selected patients with one‑sided papillary thyroid cancer. It appears to provide similar cancer control and safety to the classic open neck operation, while offering better scar appearance and somewhat more comfortable swallowing afterward—albeit with longer operating times and higher costs. The authors caution that careful pre‑surgery imaging and surgeon experience are essential, especially to judge lymph node involvement and to protect the tiny parathyroid glands. Larger studies that follow patients for many years will be needed to confirm how this approach performs over the long term, but for now it offers an appealing alternative for people who value both cancer cure and a less visible reminder of their disease.
Citation: Yang, R., Han, P., Ma, C. et al. Gasless endoscopic thyroidectomy via the trans-subclavian approach versus conventional open thyroid surgery for unilateral thyroid cancer. Sci Rep 16, 12304 (2026). https://doi.org/10.1038/s41598-026-42491-2
Keywords: thyroid cancer surgery, endoscopic thyroidectomy, minimally invasive surgery, surgical scarring, quality of life