Clear Sky Science · en
Impact of central venous pressure trajectories on prognosis in ICU patients with sepsis
Why this matters for patients with severe infections
When a person develops sepsis, a life-threatening reaction to infection, doctors must quickly give fluids and medicines to support the heart and circulation. One common bedside measurement is central venous pressure (CVP), the pressure inside large veins near the heart. This study asked a simple but crucial question: if we track how CVP changes over the first day in the intensive care unit, can those patterns tell us who is more likely to survive?
Following blood pressure inside big veins
CVP is measured through a thin tube placed in a large vein leading to the heart. For decades it has been used as a rough guide to how much fluid to give very sick patients, including those with sepsis. Yet research has shown that a single CVP reading is a poor predictor of whether the heart will actually pump better if more fluid is given. Rather than looking at one snapshot, the authors used a large hospital database called MIMIC-IV, containing detailed records from tens of thousands of ICU stays, to follow how CVP changed over the first 24 hours in adults with sepsis and then linked those patterns to survival.
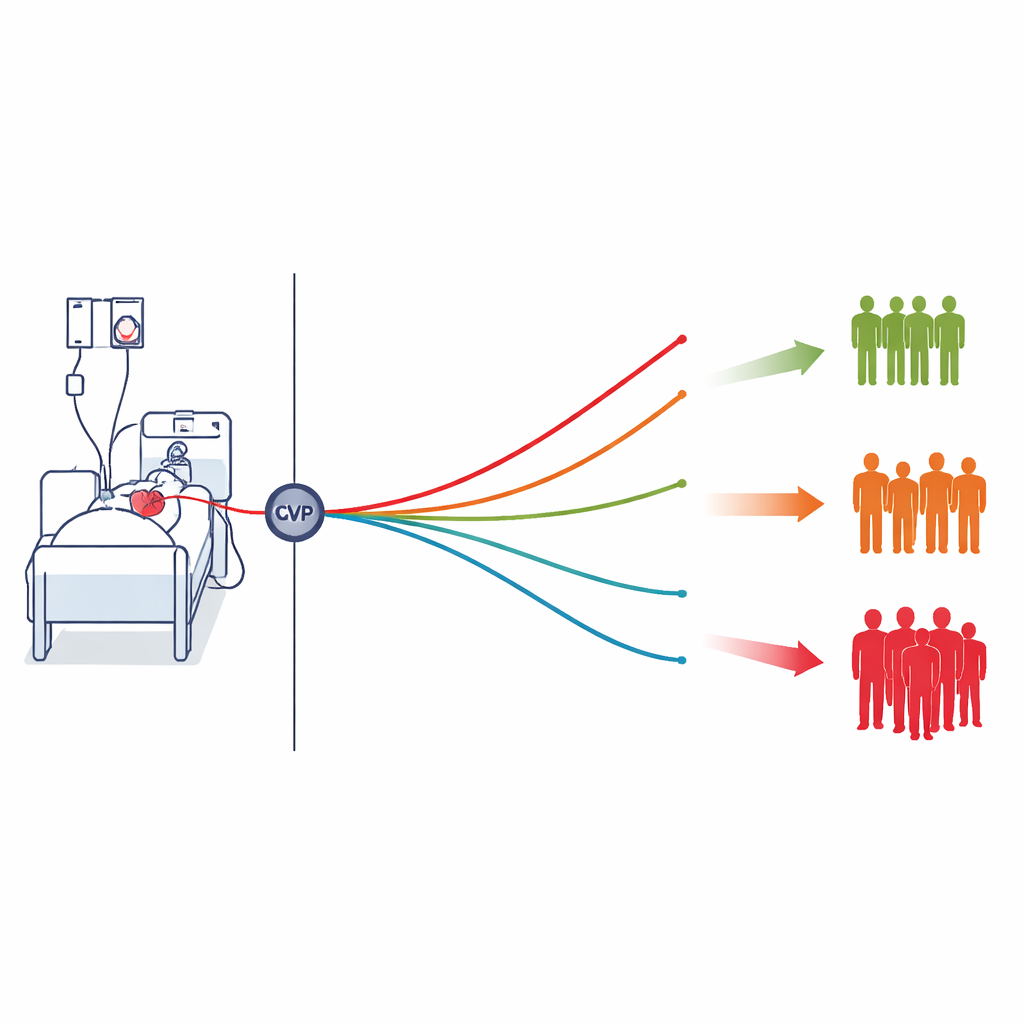
Four patterns of vein pressure over time
The team analyzed data from 3,068 septic patients who had CVP measured repeatedly in the first ICU day. Using a statistical approach called group-based trajectory modeling, they grouped patients with similar CVP trends into four patterns. One group had low CVP that gradually declined; a second started at moderate levels and slowly fell; a third began high and drifted down; and a fourth had persistently high CVP that actually rose over time. Each group included at least a twentieth of the patients, and the modeling showed that individuals were assigned to their group with high confidence.
Linking pressure patterns to chances of survival
When the researchers compared outcomes across these four patterns, clear differences emerged. Patients whose CVP stayed low and declined had the lowest risk of dying in the ICU and in the hospital, and they also had better survival up to one year. Those with high CVP that declined over time were more than twice as likely to die in the ICU, even after accounting for age, illness severity, underlying heart disease, and many laboratory results. The group with persistently high and rising CVP fared worst of all, with more than four times the ICU death risk of the low group. These trends held up in multiple sensitivity checks and in subgroups such as patients on ventilators or with heart rhythm problems.
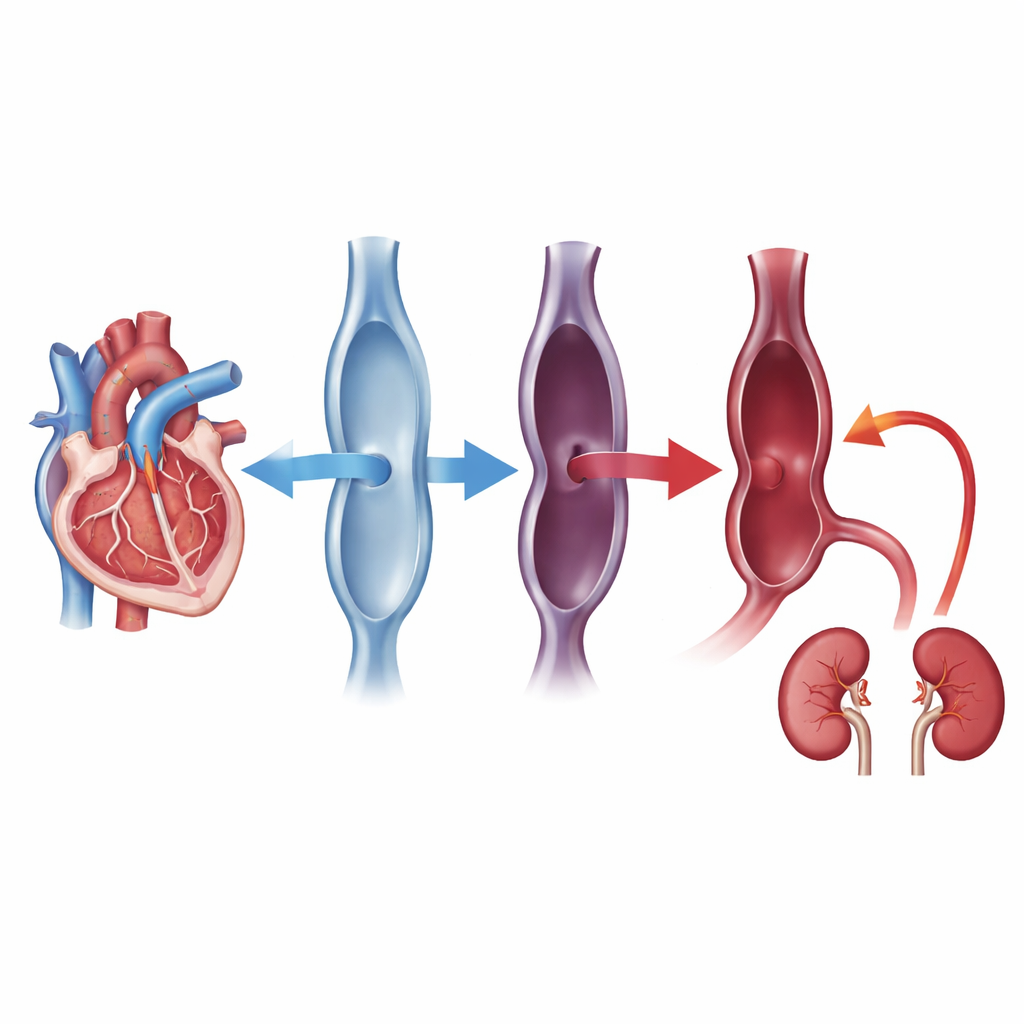
What rising vein pressure may really be telling us
The authors argue that CVP should not be viewed simply as a measure of how full the circulation is. Instead, it reflects a complex balance between the blood returning to the heart, how well the right side of the heart pumps, and pressures inside the chest. In sepsis, stiff blood vessels, leaky capillaries, lung injury, and weak heart function can all drive CVP up even when total blood volume is not excessive. Persistently high or rising CVP, they suggest, may signal that the heart and veins are struggling, leading to congestion in organs such as the kidneys. In fact, the study found that patients in the higher CVP groups had more acute kidney injury, supporting this idea of harmful back-pressure within the body.
How this could change care at the bedside
This work does not prove that high CVP directly causes organ damage or death, but it strengthens the case for using CVP trends as an early warning sign rather than as a simple fluid target. For clinicians, the message is to be cautious when CVP climbs and stays high during the first ICU day in sepsis: further fluid loading may offer little benefit and could worsen congestion. Instead, doctors may need to focus more on heart function, pressures in the chest, and ways to relieve venous buildup. For patients and families, the takeaway is that continuous, thoughtful monitoring of these pressures can provide valuable clues about risk and may help tailor treatment to the individual needs of each person with sepsis.
Citation: Chen, J., Que, S., Jin, G. et al. Impact of central venous pressure trajectories on prognosis in ICU patients with sepsis. Sci Rep 16, 11486 (2026). https://doi.org/10.1038/s41598-026-41213-y
Keywords: sepsis, central venous pressure, intensive care, fluid resuscitation, kidney injury