Clear Sky Science · en
Tumor mutations predict HER2-targeted therapy resistance in primary HER2-positive breast cancer
Why some breast tumors refuse to back down
For many people with an aggressive form of breast cancer called HER2‑positive disease, modern drugs that precisely target the HER2 protein have transformed outcomes. Yet doctors still see a puzzling pattern: some tumors melt away before surgery, while others barely budge despite the same powerful treatment. This study asked a simple but crucial question—can tiny DNA changes inside the tumor help explain who responds and who does not?
Looking inside tumors for hidden clues
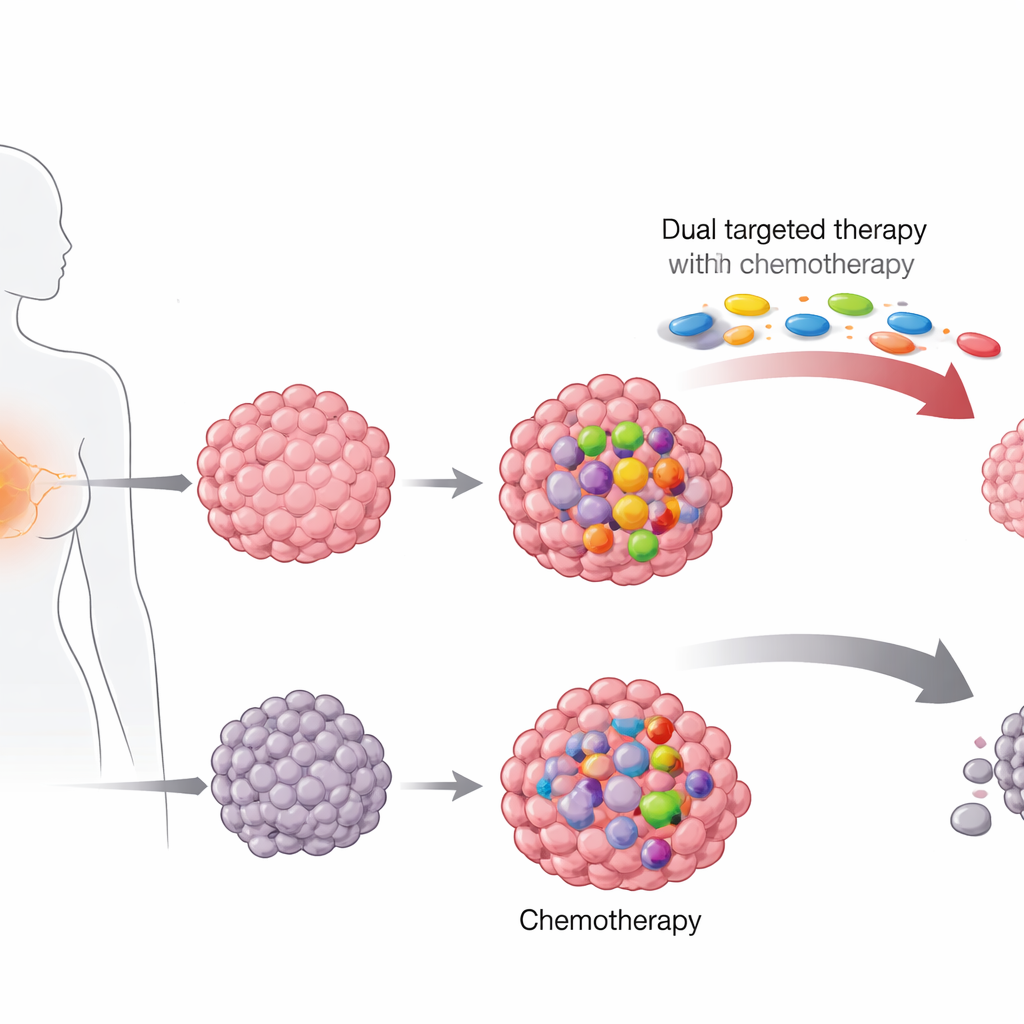
The researchers examined stored biopsy samples from 364 women with HER2‑positive breast cancer who had taken part in two large treatment trials in Germany. One trial, run before HER2‑targeted drugs were common, tested different chemotherapy combinations alone. The more recent trial added a “dual blockade” of HER2 using two drugs, trastuzumab and pertuzumab, on top of chemotherapy with taxane drugs and anthracyclines. Using next‑generation DNA sequencing, the team searched each tumor for hot‑spot mutations in 17 genes often altered in breast cancer, focusing especially on PIK3CA and TP53.
Common genetic changes in HER2‑positive disease
Nearly two‑thirds of the tumors carried at least one important mutation. Changes in TP53, a gene that normally acts as a brake on damaged cells, were the most frequent, found in almost half of the cancers. Mutations in PIK3CA, which switch on a growth‑promoting pathway inside the cell, appeared in about one quarter of tumors. A small fraction also had mutations in genes linked to another major signaling route, the MAPK pathway. Many tumors carried more than one alteration, and PIK3CA changes often traveled together with TP53 or MAPK‑related mutations, suggesting multiple growth advantages layered within the same cancer.
Which mutations matter for treatment response?
The team then compared these genetic findings with how completely each tumor disappeared after therapy, a benchmark known as pathological complete response. In the newer trial that used dual HER2 blockade, patients whose tumors lacked PIK3CA mutations were much more likely to achieve this deep response than those whose tumors carried the mutation. About two‑thirds of women with PIK3CA‑normal tumors had no cancer left at surgery, versus less than half of those with PIK3CA‑mutant disease. This gap remained even after accounting for factors such as tumor size, hormone‑receptor status, and cell growth rate. In contrast, TP53 and MAPK‑related mutations did not show a meaningful link with treatment success.
Clues from different chemotherapy backbones
The picture grew sharper when the researchers examined specific chemotherapy drugs. In the dual‑blockade trial, patients were randomly assigned to receive standard paclitaxel or a more concentrated formulation called nab‑paclitaxel before surgery. Among women given nab‑paclitaxel, PIK3CA mutations were strongly tied to poor tumor clearing: fewer than four in ten mutant tumors vanished, compared with more than seven in ten without the mutation. This difference almost disappeared in the paclitaxel group, hinting that the high‑dose, cell‑division‑targeting action of nab‑paclitaxel may unintentionally favor survival of PIK3CA‑mutant cells. Strikingly, in the older trial where patients received chemotherapy alone without HER2‑targeted drugs, PIK3CA status did not significantly influence response, suggesting that the mutation’s main impact emerges when the HER2 signal is blocked.
What these findings mean for patients
For people facing HER2‑positive breast cancer, the study offers a clearer explanation for why some tumors resist even intensive, modern treatment. Tumors with PIK3CA mutations seem able to bypass the HER2 blockade by switching on a parallel growth engine inside the cell, and they may also better withstand certain forms of chemotherapy. While the study was not large enough to prove major differences in long‑term survival, its results strongly support using PIK3CA status as a guide when planning therapy. In the future, combining HER2‑targeted drugs with medicines that shut down the PIK3CA pathway—or avoiding nab‑paclitaxel in mutation‑positive tumors—could help turn more partial responses into complete ones, giving patients a better chance that their cancer will not return.
Citation: Van Mackelenbergh, M.T., Pfarr, N., Weber, K. et al. Tumor mutations predict HER2-targeted therapy resistance in primary HER2-positive breast cancer. npj Breast Cancer 12, 59 (2026). https://doi.org/10.1038/s41523-026-00948-7
Keywords: HER2-positive breast cancer, PIK3CA mutation, targeted therapy resistance, neoadjuvant chemotherapy, tumor genomics