Clear Sky Science · en
PD-1 blockade plus tyrosine kinase inhibitor remodels the tumor microenvironment in advanced renal cell carcinoma
Why kidney cancer treatment can stop working
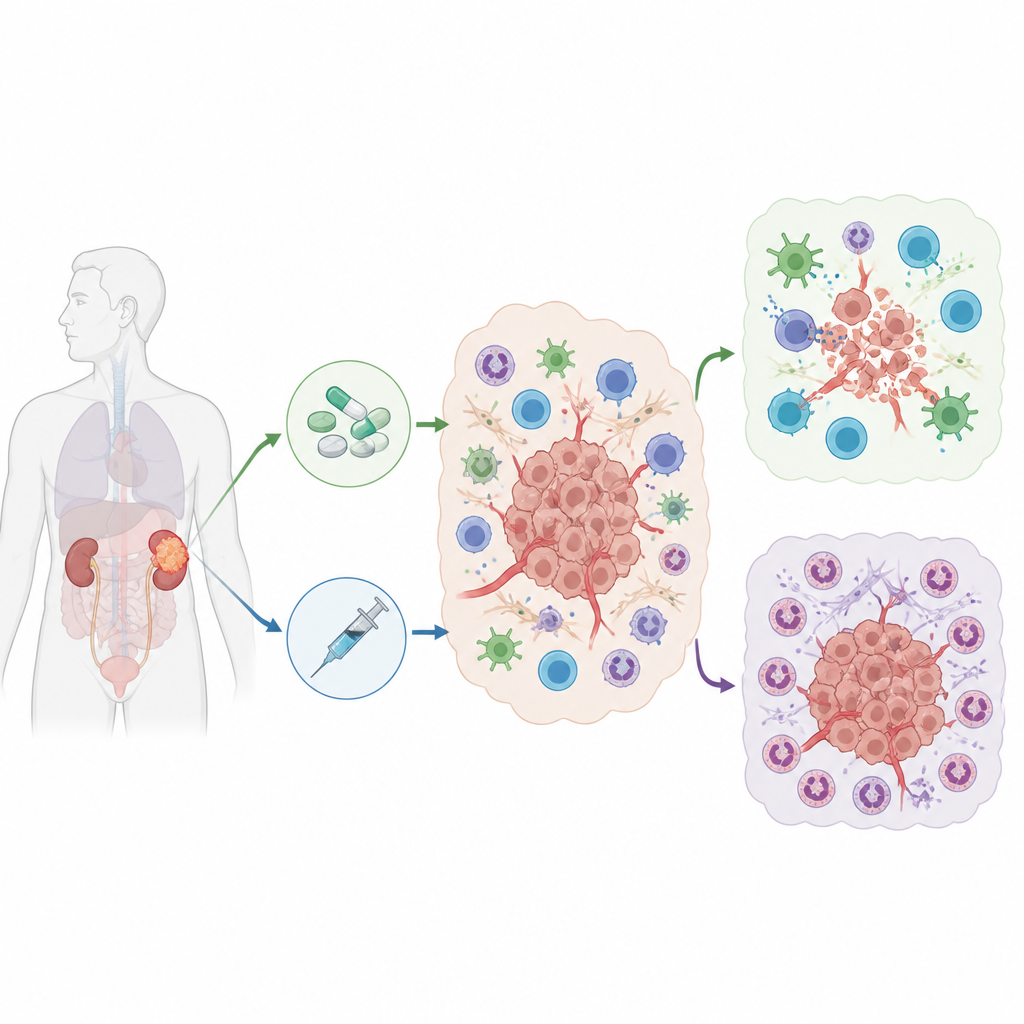
Many people with advanced kidney cancer now receive a powerful drug duo: one medicine that cuts off the tumor’s blood supply and another that helps the immune system attack. Yet a troubling number of patients see their cancer stop responding. This study asks a simple but crucial question: what inside the tumor helps some patients benefit from this combination while others relapse or never respond at all?
The neighborhood around the tumor
Cancers do not grow in isolation; they live in a busy neighborhood of immune cells, blood vessels, and supporting tissue known as the tumor microenvironment. The researchers collected 61 tumor samples from 34 people with advanced kidney cancer who had been treated with blood vessel–blocking drugs, immune drugs, or both. Using single-cell RNA sequencing, a technique that reads the activity of thousands of genes in individual cells, they built a detailed map of nearly 333,000 cells. This map showed many cell types, including cancer cells, T cells that can kill tumors, and several kinds of white blood cells that can either help or hinder the immune attack.
Helpful and harmful immune cells
When the team compared patients who responded to treatment with those who did not, they found clear patterns. Responders tended to have more T cells inside their tumors and fewer cells from a group called myeloid cells, which includes macrophages and neutrophils. Non-responders showed the opposite pattern, especially after combination therapy. A closer look at neutrophils, a type of fast-acting white blood cell, revealed several distinct subgroups. One subgroup, marked by strong signals related to blood vessel growth and low-oxygen metabolism, expanded sharply in non-responders after treatment. These neutrophils were linked to poor outcomes and signs of blocking T cell activity.
A signal from cancer cells that recruits suppressors
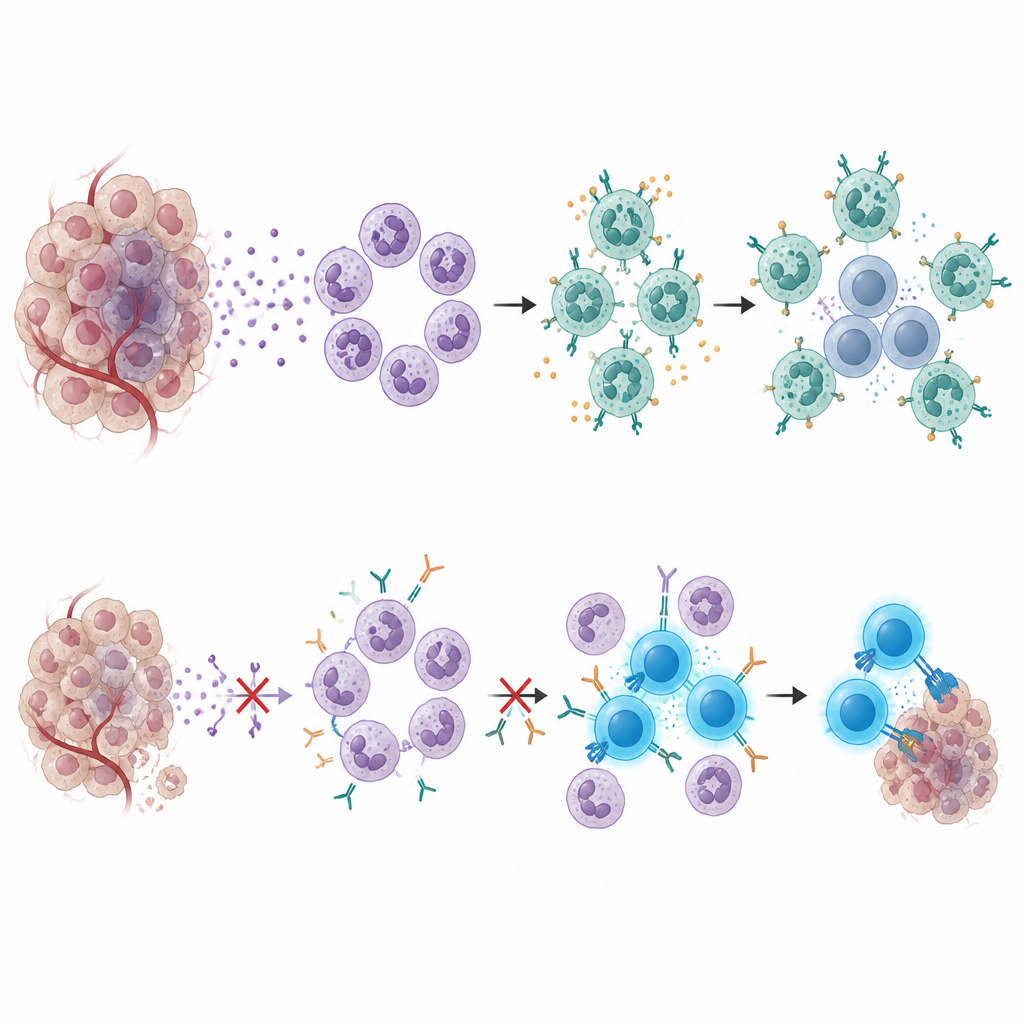
The cancer cells themselves played a key role in attracting these harmful neutrophils. In tumors from non-responders, cancer cells turned on genes related to inflammation and the recruitment of neutrophils. Two of these genes produce a protein called serum amyloid A (SAA), a molecule usually seen in strong inflammatory reactions. Tumors rich in SAA-expressing cells were more common in patients who resisted therapy, and higher SAA levels in blood samples before treatment were tied to worse survival. Across several cancer datasets, patients with high SAA levels tended to fare more poorly on immune-based treatments, suggesting that SAA marks a stubborn, treatment-resistant tumor state.
A communication loop that shuts down T cells
By combining cell maps, spatial data, and mouse experiments, the scientists pieced together a communication loop. SAA released by tumor cells drives neutrophils toward a suppressive state that produces VEGFA and a surface protein called CEACAM1. These neutrophils often cluster near a subset of CD8 T cells that display another checkpoint protein called TIM-3. Signals passing from CEACAM1 on neutrophils to TIM-3 on T cells push the T cells into exhaustion, leaving them unable to eliminate cancer cells even in the presence of PD-1–blocking drugs. In mice, blocking SAA made tumors more sensitive to the drug combination and reduced neutrophil buildup, while blocking the CEACAM1–TIM-3 interaction, especially together with PD-1 inhibition, restored T cell activity and slowed tumor growth.
New targets to keep treatments working longer
To a non-specialist, the message of this study is that some kidney tumors escape modern combination therapy by building a protective shield of specialized neutrophils and exhausted T cells. A tumor-made protein, SAA, summons and shapes these neutrophils, which then silence nearby T cells through a CEACAM1–TIM-3 brake. Measuring SAA in blood could help flag patients at high risk of resistance, and drugs that block SAA or the CEACAM1–TIM-3 link may one day be added to current regimens. By disrupting this hidden immune escape route, future treatments could give more patients a lasting benefit from kidney cancer immunotherapy.
Citation: Gu, L., Zhang, Q., Liang, Q. et al. PD-1 blockade plus tyrosine kinase inhibitor remodels the tumor microenvironment in advanced renal cell carcinoma. Nat Commun 17, 4626 (2026). https://doi.org/10.1038/s41467-026-70978-z
Keywords: renal cell carcinoma, tumor microenvironment, neutrophils, immune checkpoint therapy, treatment resistance