Clear Sky Science · en
RIP kinase inhibition with Necrostatin-1 improves human marginal mass islet graft survival and function for the management of type 1 diabetes
Helping Donor Cells Survive in Diabetes Treatment
For people with type 1 diabetes, one experimental option is to transplant clusters of insulin-making cells, called islets, from donor organs. These tiny cell clusters can restore natural blood sugar control, but many of them die soon after transplant, so patients often need islets from several donors. This study tests a short, targeted treatment that aims to keep more of those fragile donor cells alive, with the hope of making single-donor transplants more realistic.
Why Islet Transplants Lose So Many Cells
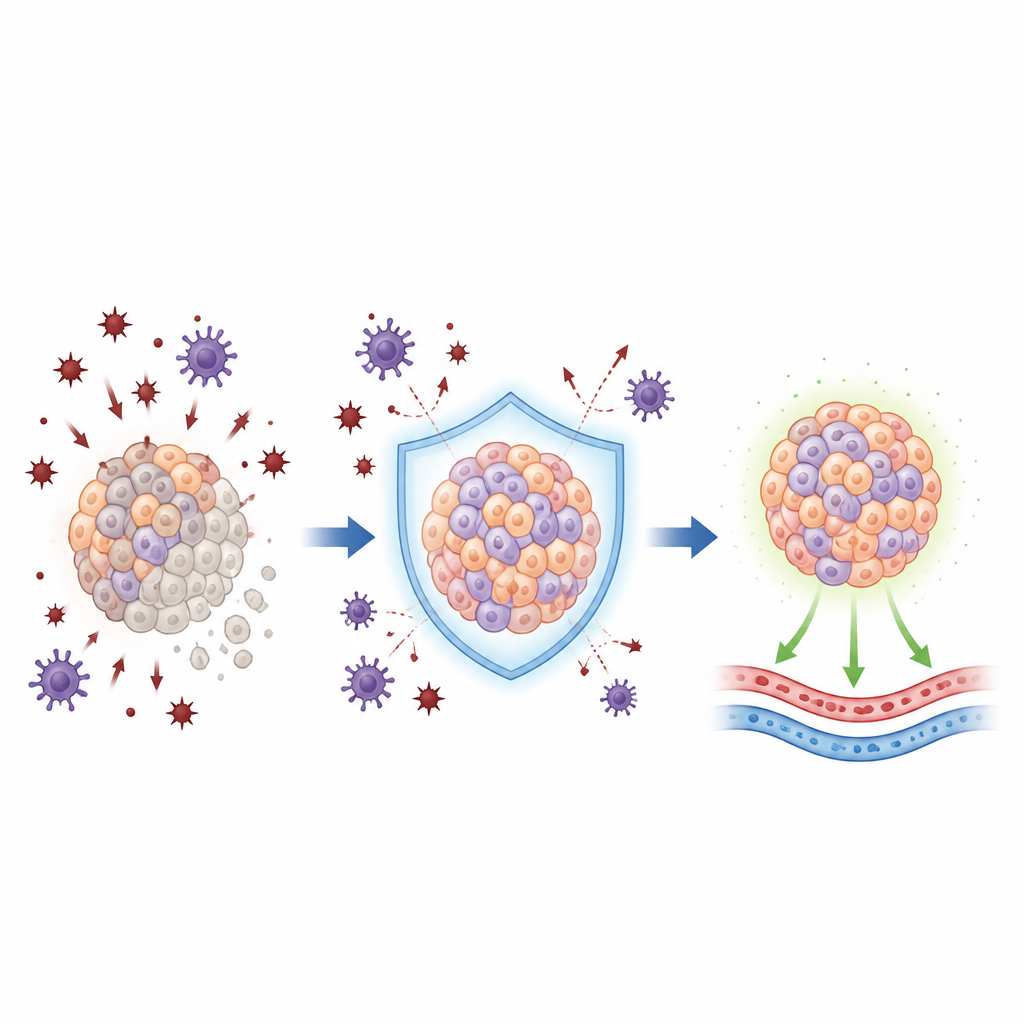
When islets are removed from a donor pancreas, handled in the lab, and then placed into a recipient, they experience a storm of stress. Inflammation, low oxygen, and chemical damage can trigger different forms of cell death. Past efforts mainly focused on blocking one form, apoptosis, sometimes called “programmed cell suicide.” But another form of cell death, closer to a controlled version of bursting or necrosis, also seems to play an important role. That process is driven by a group of proteins known as RIP kinases, which act like switches that decide whether stressed cells recover or fall apart.
A Short Protective Bath for Donor Islets
The researchers explored whether giving donor islets a 24-hour “bath” in the lab with a drug called Necrostatin-1 could tip the balance toward survival. Necrostatin-1 blocks a key RIP kinase, RIPK1, and is known to interfere with several stress pathways inside cells. Human islets from organ donors were split into groups and exposed either to Necrostatin-1, a more stable cousin of the drug, or a standard apoptosis blocker, then kept in culture under conditions that normally lead to gradual cell loss. The team measured how many cells died, how many insulin-producing cells remained, how well they released insulin in response to sugar, and how efficiently they used oxygen.
What Happened to the Treated Cells
Islets pre-treated with Necrostatin-1 showed fewer dying cells and more surviving insulin-producing cells than untreated controls, and they performed at least as well as those given the apoptosis blocker. Their ability to release insulin in response to glucose remained intact. At the genetic level, Necrostatin-1 powerfully dialed down many inflammation-related pathways, including those driven by immune messengers and tissue remodeling signals. In other words, a brief exposure before transplant appeared to quiet stress signals inside the islets while preserving their basic identity and function. The more stable cousin drug had weaker and less consistent effects, suggesting that Necrostatin-1’s particular mix of actions matters.
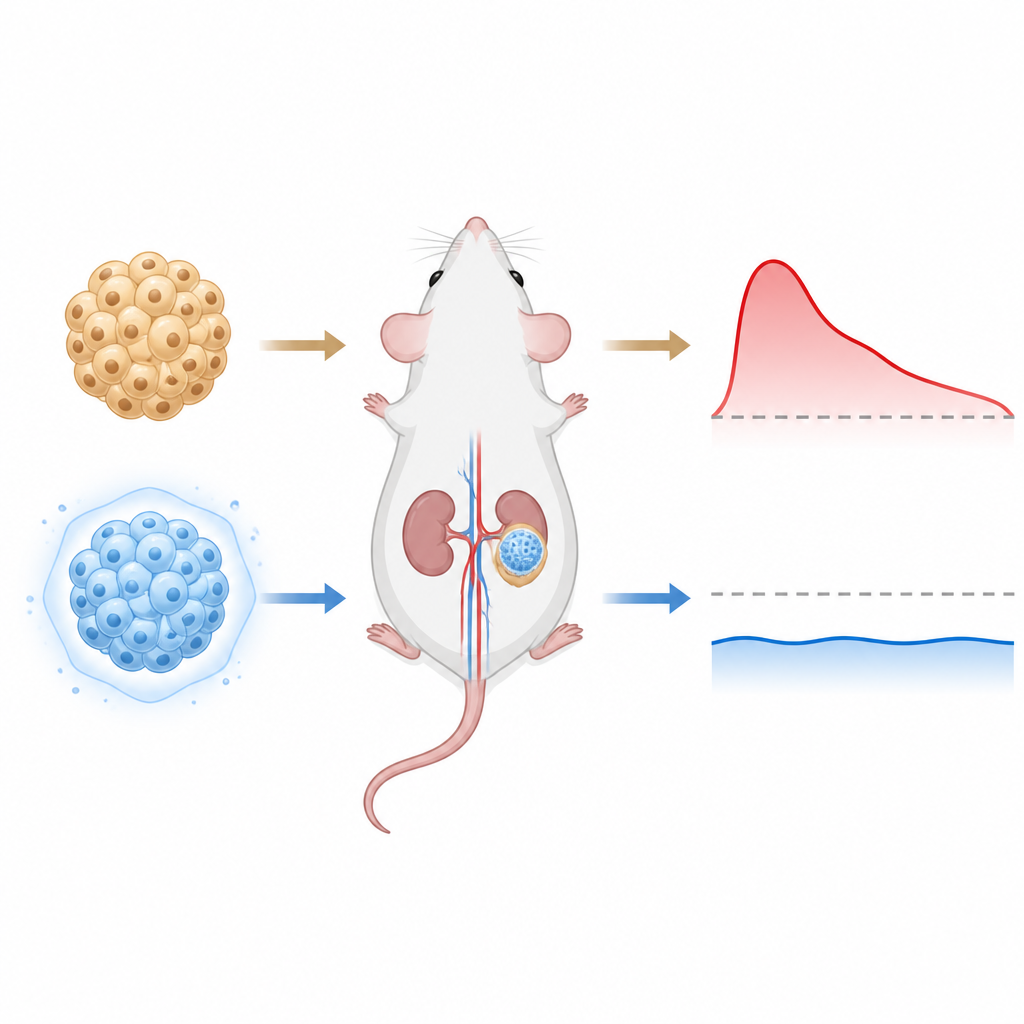
Testing Transplants in Diabetic Mice
The team then asked the crucial question: would this brief treatment actually improve transplant success in living animals? They transplanted a “marginal” number of human islets, just enough that survival really matters, under the kidney capsule of diabetic mice. Untreated islets rarely managed to bring blood sugar down in this challenging setup. In contrast, islets pre-treated with Necrostatin-1 reliably restored normal sugar levels in all recipient mice, and they did so faster and more completely than controls. When the researchers later removed the graft-bearing kidney, the animals quickly became diabetic again, confirming that the protected islets were responsible for the improved control. Early gene activity patterns in the grafts showed that Necrostatin-1 had shifted the tissue toward a calmer, more balanced state, with more survival signals and fewer danger messages.
What This Could Mean for People with Diabetes
This work suggests that giving donor islets a short, carefully timed treatment before transplant can help more of them survive the stressful early days in their new home. By reducing cell death and dialing down harmful inflammation, Necrostatin-1 pre-treatment allowed a relatively small number of human islets to control diabetes in mice long term. While more research is needed before this approach can be tested in people, especially in more realistic transplant sites, the idea is straightforward: protect donor cells at their most vulnerable moment so that fewer are needed overall. If similar benefits hold in human patients, this strategy could make islet transplants more efficient and potentially open the door for single-donor cell therapy for type 1 diabetes.
Citation: Aggarwal, S., Cuesta-Gomez, N., Paramor, J. et al. RIP kinase inhibition with Necrostatin-1 improves human marginal mass islet graft survival and function for the management of type 1 diabetes. Cell Death Dis 17, 501 (2026). https://doi.org/10.1038/s41419-026-08728-8
Keywords: islet transplantation, type 1 diabetes, cell death pathways, RIPK1 inhibition, beta cell survival