Clear Sky Science · en
Divergent clonal evolution and tumor microenvironment remodeling shape gastric cancer peritoneal metastasis
Why this study matters
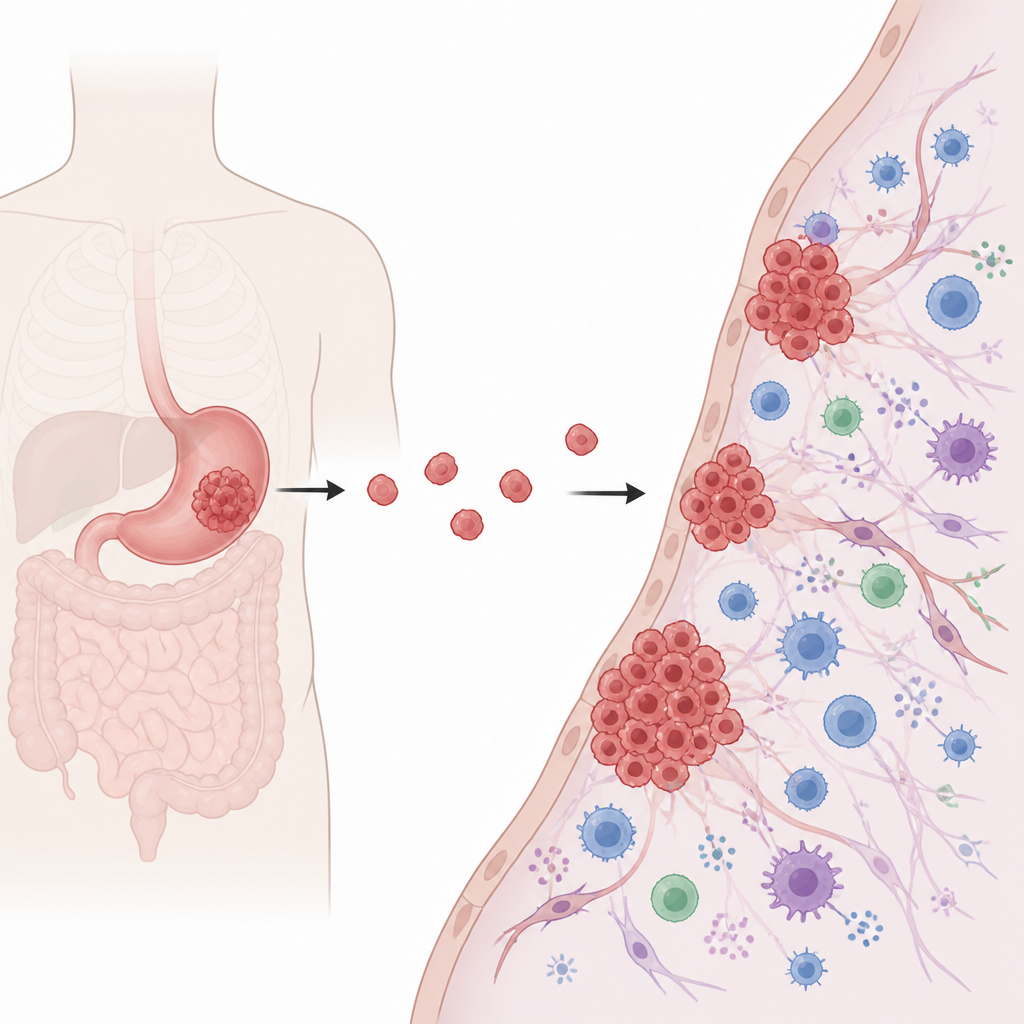
When stomach cancer spreads into the abdominal cavity, it often coats the inner lining with countless tiny tumors. This form of spread, called peritoneal metastasis, is common, hard to detect, and usually deadly within a year. Standard drugs and new immunotherapies rarely work well in these patients. This study asks a simple but crucial question: are these scattered tumor deposits fundamentally different from the original stomach tumor, and could that explain why current treatments fail?
Following cancer from the stomach to the abdomen
The researchers collected tissue from 26 people with advanced stomach cancer whose disease had spread to the peritoneum. For many patients they had both the primary stomach tumor and matching metastatic samples, along with some nearby normal tissue. They read out the complete DNA and activity of thousands of genes in these samples. By comparing genetic changes and patterns of gene use across sites, they could track how cancer cells evolve as they leave the stomach, seed the peritoneal lining, and adapt to their new niche.
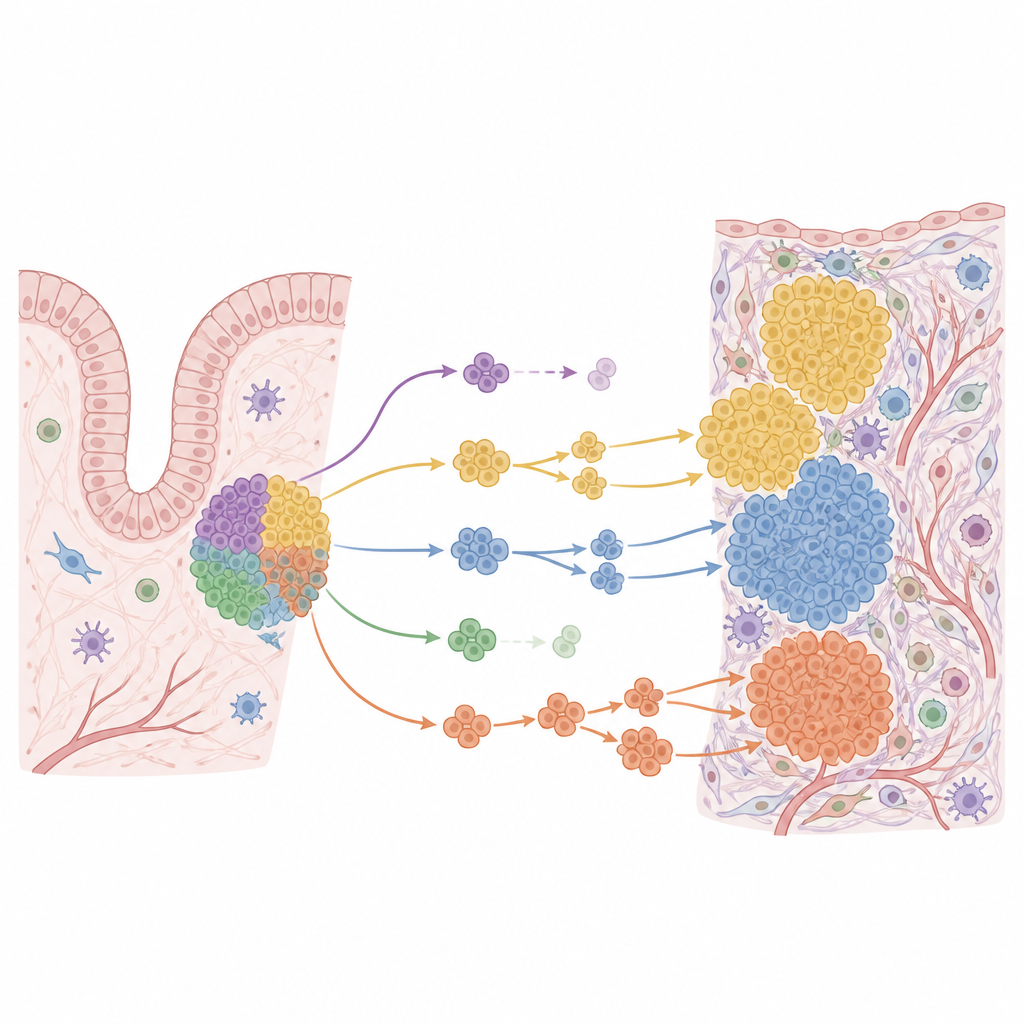
Many routes, not one, to deadly spread
The team found that there is no single genetic blueprint for this type of spread. Within a single patient, the original tumor and the peritoneal metastases often shared only part of their mutation set, and in some cases very little at all. In general, the metastatic deposits carried fewer point mutations than the primary tumors, but more complex DNA rearrangements. Some cancer-driving genes were altered only in the primary tumor, others only in the metastases. By reconstructing family trees of cancer cell clones, the authors showed that, in most patients, the primary tumor and peritoneal deposits branched apart early and then followed separate evolutionary paths.
Primary tumors that already look like metastases
When the scientists focused on which genes were turned on or off, they saw a spectrum from normal stomach tissue to primary tumors to peritoneal metastases. Many primary tumors clustered near normal tissue, but a small subset of primaries already looked, at the gene expression level, very similar to peritoneal deposits. These tumors showed strong signs of a cellular program called epithelial to mesenchymal transition, which helps cells loosen their attachments and move, as well as heightened growth signals. In several of these cases, the primary tumors carried changes in well-known gatekeeper genes that help control cell behavior, supporting the idea that some stomach cancers are “born” with a higher tendency to seed the abdomen.
A changing neighborhood around the tumor
The study also mapped how the mix of surrounding noncancerous cells changes during spread. Using computational methods fed with single-cell data, the authors estimated the proportions of immune cells, structural cells, and other components in each sample. Primary stomach tumors were often “desert like,” with relatively few active immune cells. In contrast, many peritoneal metastases were richer in immune and scar like cells, including certain macrophages and cancer associated fibroblasts. Naive killer T cells were more common, while mature antibody producing cells were reduced, hinting at an immune system that is present but not fully effective.
Why drugs may not reach the target
These immune rich metastases raise a puzzle: if the peritoneal tumors sometimes have features linked to response to immunotherapy, why do patients with this pattern of spread rarely benefit from drugs like checkpoint inhibitors given into the bloodstream? The authors suggest that the barrier separating the blood from the peritoneal cavity may prevent enough drug from reaching these deposits. Their findings point toward treatment strategies that specifically target the peritoneal space, such as delivering chemotherapy or immunotherapy directly into the abdomen, guided by the molecular features of the metastatic tumors rather than those of the original stomach tumor.
What this means for patients
In plain terms, this work shows that the scattered tumors on the abdominal lining are not mere copies of the main stomach tumor. They have their own genetic quirks and sit in a reshaped neighborhood of immune and support cells. Some primary tumors already carry the hallmarks of this advanced state, while others evolve toward it later. Because of this diversity, and because standard drugs may not easily cross into the peritoneal cavity, the authors argue that doctors should treat peritoneal metastases as a distinct problem. Tailored testing and peritoneal focused therapies may be needed if we want to improve survival for patients facing this particularly dangerous form of stomach cancer.
Citation: Charton, C., Kang, S.H., Kim, S.S. et al. Divergent clonal evolution and tumor microenvironment remodeling shape gastric cancer peritoneal metastasis. Commun Biol 9, 666 (2026). https://doi.org/10.1038/s42003-026-09906-2
Keywords: gastric cancer, peritoneal metastasis, tumor microenvironment, clonal evolution, immunotherapy