Clear Sky Science · en
Managing the aftermath: complications and outcome after colorectal resection for deep infiltrating endometriosis—insights from a certified surgical endoscopy center
Why this matters for women’s health
For many women, endometriosis means years of pain, bowel problems, and difficulty getting pregnant. When this condition burrows deeply into the bowel, surgery can be the only way to relieve symptoms—but it also carries real risks, including leaks where the intestine is rejoined and the need for a temporary stoma (an opening on the belly for stool). This study follows more than 100 women treated at a specialized center and shows how careful planning plus modern endoscopic (from the inside) care can keep the bowel working well in the long run.
Understanding a hidden bowel disease
Endometriosis happens when tissue similar to the uterine lining grows elsewhere in the body. In its deep form, it can invade structures in the pelvis, including the rectum and sigmoid colon. Women may suffer from painful periods, pain during sex, painful bowel movements, bleeding from the rectum, urinary symptoms, and infertility. Many have already undergone more than one operation before reaching a referral center. In this study, 118 women with bowel-invading endometriosis, most in their early thirties and many with severe disease, were treated at a university hospital using shared decision-making between gynecologic and bowel surgeons.
How the team treats bowel involvement
Before surgery, every case was discussed in an expert conference and patients received bowel imaging and a detailed explanation of possible operations and the chance of a temporary stoma. Surgeons chose among three main strategies during minimally invasive (laparoscopic) procedures: shaving the disease off the front of the rectum, cutting out a disc, or removing a bowel segment and reconnecting it. In nearly all resections, the join between bowel ends was created low in the pelvis, an area known to be prone to healing problems. The team followed a strict plan after surgery: all women had an internal camera check of the bowel join around day five, even if they felt well, to catch early leaks or narrowings. 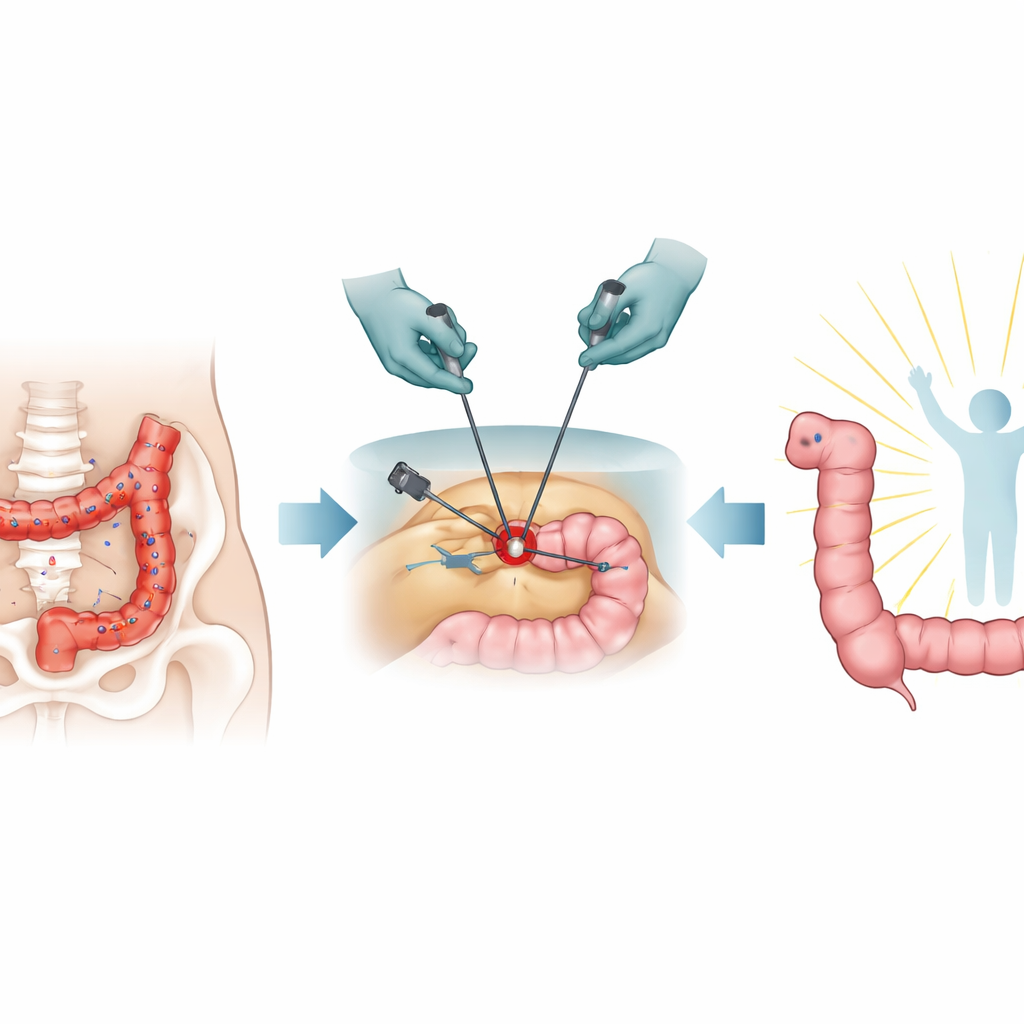
Fixing leaks and narrowings from the inside
About one in ten women developed a leak at the bowel join, and a similar number developed a narrowing. Instead of immediately re-opening the abdomen or leaving women with a permanent stoma, the center relied on endoscopic tools. For leaks, they used vacuum therapy: a sponge connected to gentle suction was placed through the anus onto the leaking area or into the small cavity beside it. This was changed every few days until the tissue grew closed. Narrowed joins were gently stretched with balloons or dilators. These procedures were mostly done without anesthesia and often as day-care visits. Impressively, all leaks healed and all temporary stomas were later reversed, preserving normal bowel continuity.
Life after surgery: function and quality of life
Years after surgery—on average more than six years—most women reported that their endometriosis-related symptoms were better than before. Those who had bowel segments removed, rather than only shaving, experienced the clearest symptom relief. Some women did develop changes in bowel habits typical after low rectal surgery, such as urgency or more frequent stools, but severe problems were limited and continence (control over bowel movements) was generally maintained. Overall health scores were good, and more than four out of five women said they would choose the same operation again. Even though a temporary ileostomy was common and often distressing, especially emotionally, every stoma created in this series was eventually taken down. 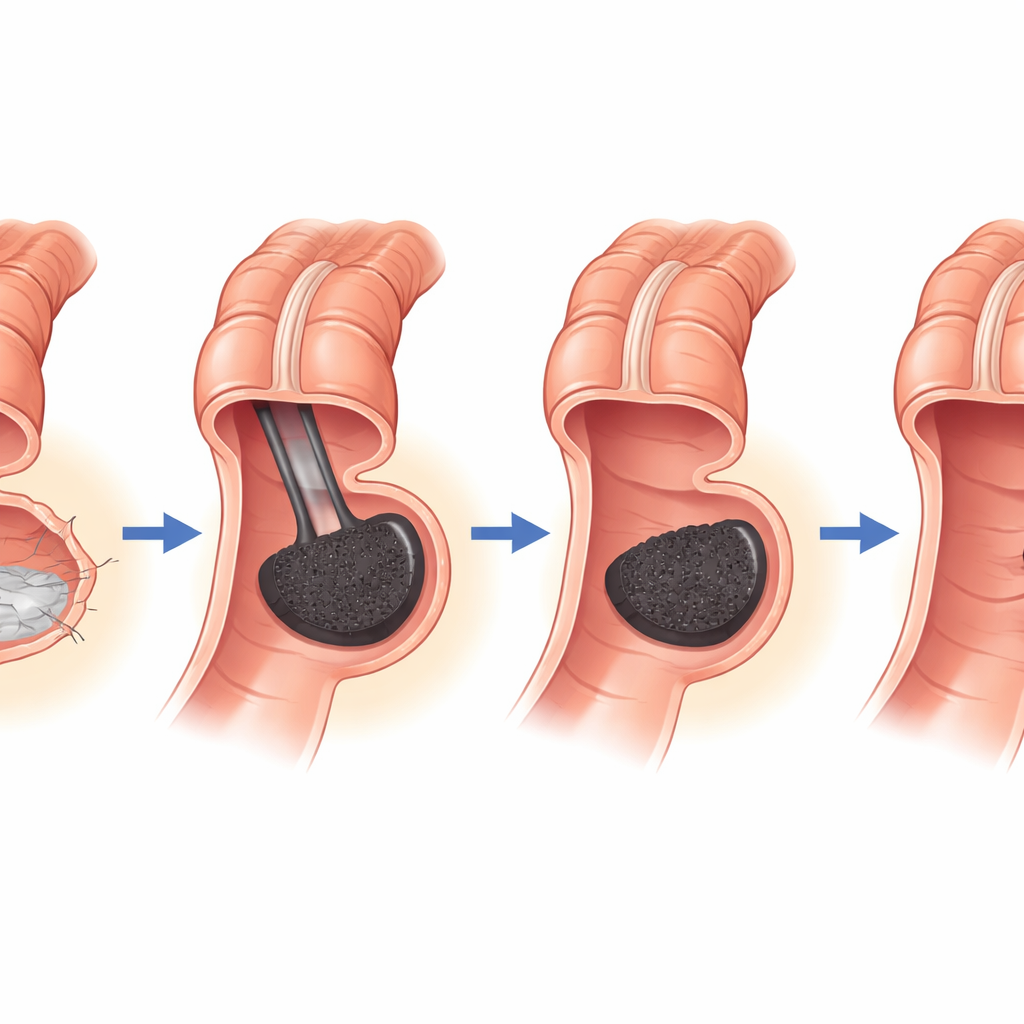
What this means for patients facing surgery
This work suggests that, when deep bowel endometriosis is handled in a specialized, team-based setting, removing the affected bowel can provide lasting symptom relief and preserve both bowel control and future fertility options. A key message is that complications such as leaks or narrowings, while not rare, do not have to mean the end of normal bowel function. With routine early endoscopic checks and proactive vacuum therapy or dilatation, surgeons can often rescue the bowel join and avoid permanent stomas. The authors argue that such structured, center-based care—and not just the choice of surgical technique—may be what truly determines long-term outcomes for young women living with this challenging disease.
Citation: Flammang, I., Eichelmann, AK., Schäfer, S. et al. Managing the aftermath: complications and outcome after colorectal resection for deep infiltrating endometriosis—insights from a certified surgical endoscopy center. Sci Rep 16, 12020 (2026). https://doi.org/10.1038/s41598-026-47171-9
Keywords: endometriosis, bowel surgery, colorectal complications, pelvic pain, fertility