Clear Sky Science · en
Efficacy of argatroban plus alteplase versus intravenous alteplase according to diabetes mellitus in acute ischemic stroke
Why this stroke study matters
Stroke is one of the leading causes of disability worldwide, and minutes can mean the difference between independence and lifelong disability. Many people with stroke also have diabetes, which can change how their blood vessels and clots behave. This study asks a practical question that matters to patients, families, and clinicians alike: when a stroke is treated with a clot busting drug, does adding a blood thinner help people with and without diabetes recover better, or does diabetes change how well this combined approach works?
How stroke is treated right now
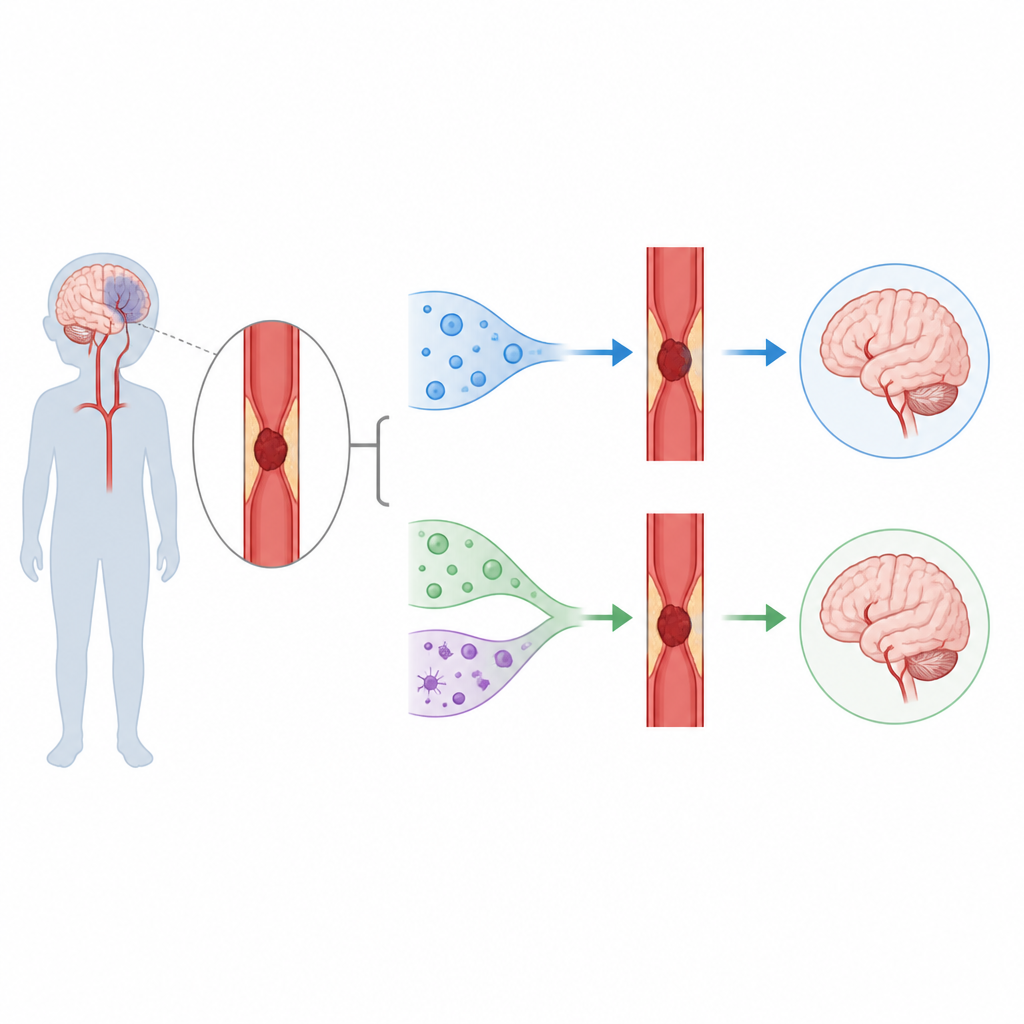
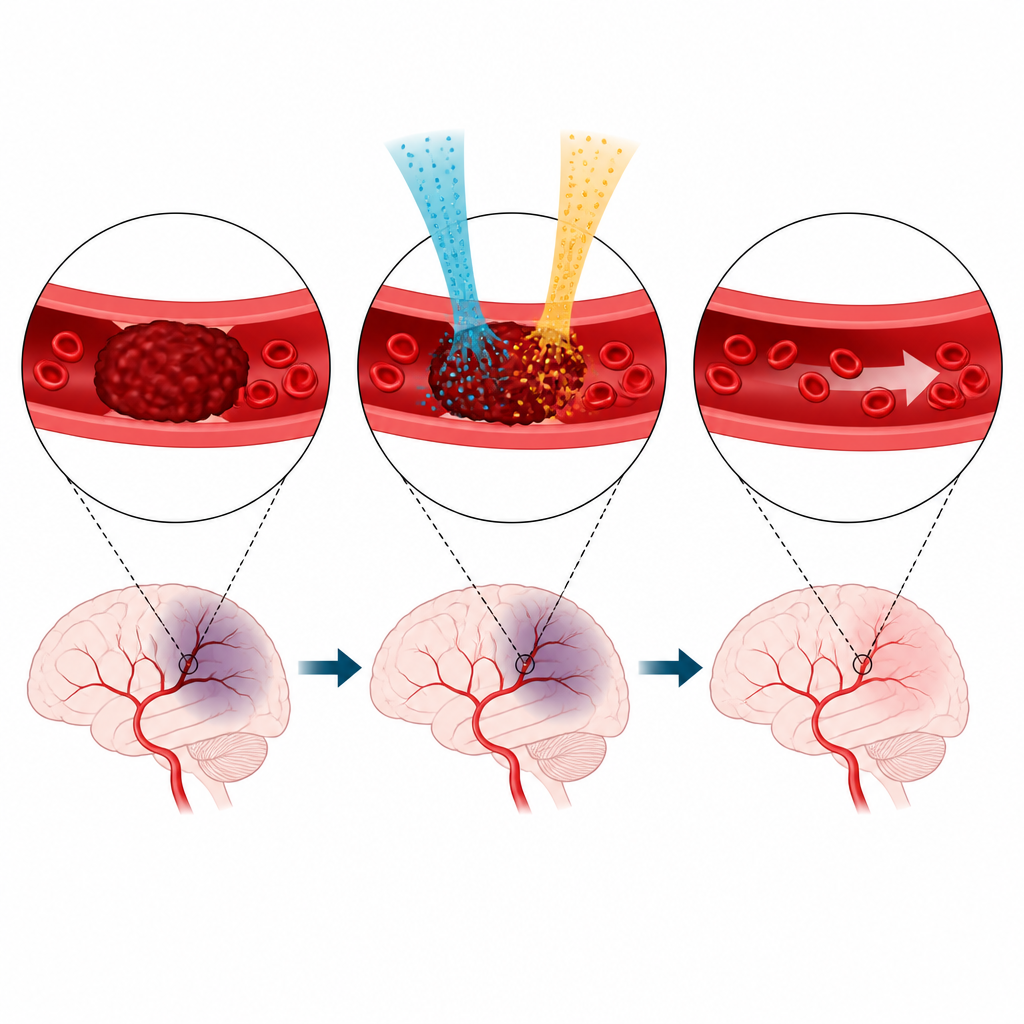
Most strokes happen when a clot suddenly blocks a blood vessel in the brain, cutting off oxygen to nearby tissue. The standard emergency treatment in the first few hours is an intravenous medicine that dissolves clots, helping restore blood flow. Some patients with large blocked arteries can also receive a mechanical procedure to pull the clot out, but this requires special equipment and trained teams that are not available everywhere. Even with the clot dissolving drug, only a fraction of patients achieve full reopening of the blocked vessel, and some vessels close off again soon after. These limits have led researchers to test whether adding carefully chosen blood thinners during this critical window might keep vessels open longer and improve recovery.
What the researchers wanted to find out
The team focused on a drug called argatroban, a direct blood thinner that targets thrombin, a key clotting protein. Earlier work in some Asian stroke populations hinted that combining argatroban with the standard clot dissolving drug might improve opening of large brain arteries without a major increase in bleeding. However, a large clinical trial called ARAIS had already shown that, overall, adding argatroban did not increase the chance of an excellent recovery compared with the clot dissolver alone. Because diabetes can change blood vessel health, clot structure, and healing after stroke, the researchers asked a more specific question: does having diabetes alter the benefit or risk of the argatroban plus clot dissolver combination compared with the clot dissolver by itself?
How the study was carried out
This work is a new analysis of data from the ARAIS trial, which enrolled adults with significant symptoms from an acute ischemic stroke within four and a half hours after onset. Everyone received the standard clot dissolving medicine. Half were randomly assigned to also receive argatroban by intravenous infusion for two days, while the other half received no additional blood thinner beyond usual care. For this analysis, the investigators divided the 696 eligible patients into two groups: 162 with diabetes and 534 without. They then compared how many people in each group were living with no symptoms or only minor symptoms three months after their stroke. They also tracked early improvement or worsening in neurologic scores, repeat strokes or other vessel problems, and different types of brain or body bleeding.
What the study found
In both people with diabetes and those without, adding argatroban did not meaningfully change the chances of excellent recovery at three months compared with the clot dissolver alone. In the diabetes group, a similar share of patients in each treatment arm regained very good function, and the small difference observed could easily have been due to chance. The same pattern held in the non-diabetes group. Measures of modest disability, early improvement, early decline, and stroke or other vessel events also looked similar regardless of whether argatroban was used. Importantly, serious safety concerns like symptomatic brain bleeding, large brain hemorrhages inside the stroke area, and major bleeding elsewhere in the body occurred at low and comparable rates in both treatment strategies, in both diabetes and non-diabetes subgroups.
What this means for patients and care teams
The findings suggest that, within the limits of this study, having diabetes does not make the combination of argatroban plus a clot dissolving drug clearly better or worse than the clot dissolver alone for early stroke treatment. In practical terms, for the types of patients enrolled in this trial, routine use of this specific drug combination cannot be recommended or rejected based solely on whether a person has diabetes. The authors note that the number of patients with diabetes was modest and that few participants had large artery blockages, where a benefit might be more likely. They conclude that while diabetes does not seem to change the overall balance of benefit and risk seen in ARAIS, larger and more targeted studies are needed before emergency stroke treatment guidelines would change.
Citation: Hou, XW., Cui, Y., Zhang, NN. et al. Efficacy of argatroban plus alteplase versus intravenous alteplase according to diabetes mellitus in acute ischemic stroke. Sci Rep 16, 15963 (2026). https://doi.org/10.1038/s41598-026-47016-5
Keywords: acute ischemic stroke, alteplase, argatroban, diabetes, stroke treatment