Clear Sky Science · en
The value of the monocyte-to-lymphocyte ratio and osteopontin (SPP1) in tuberculosis treatment response monitoring
Why tracking TB in the blood matters
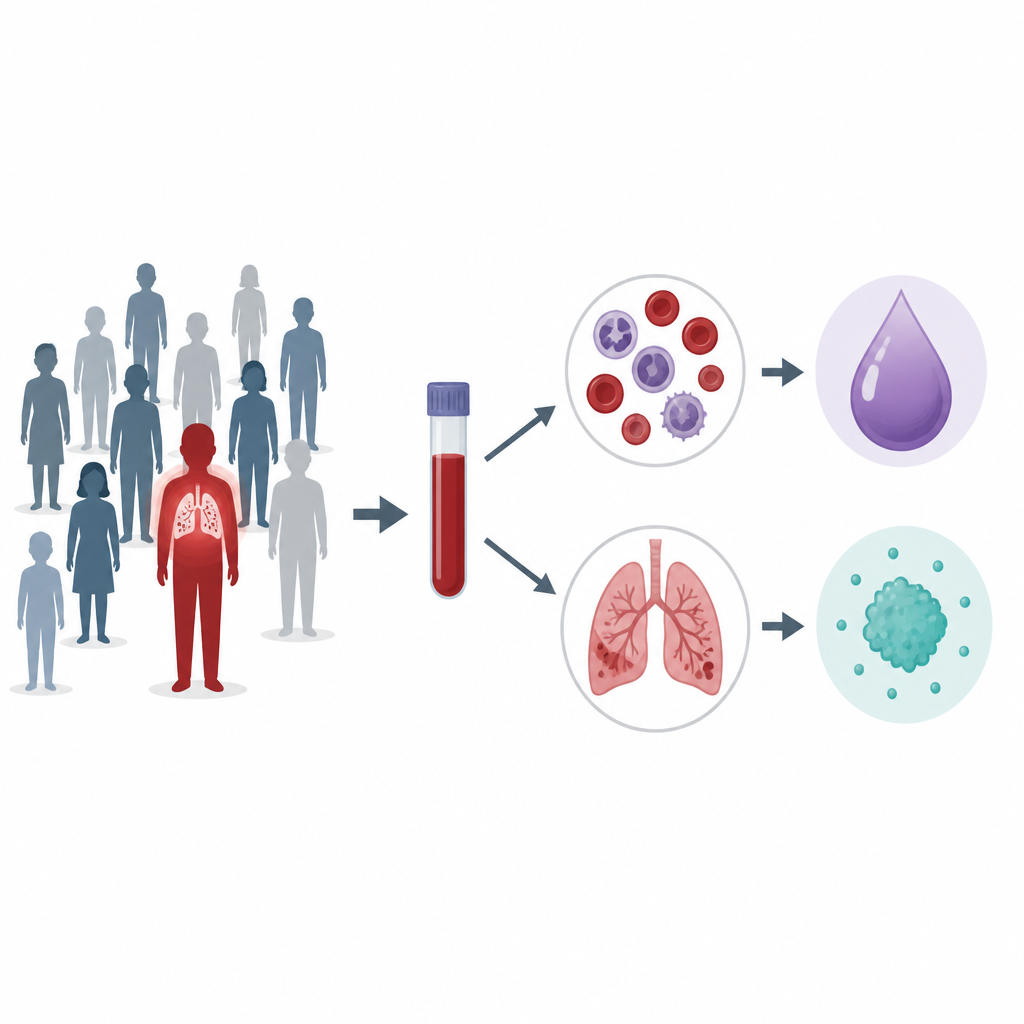
Tuberculosis remains one of the world’s deadliest infections, and doctors still struggle to tell quickly whether treatment is working. Today this often requires waiting weeks for sputum cultures from lung samples, which is slow, costly, and not always possible, especially in children or people who cannot produce sputum. This study explored whether simple blood-based signals from the immune system could help flag active tuberculosis and track how patients respond to standard drug treatment over six months.
A closer look at the people in the study
The researchers worked with adults from communities around Cape Town in South Africa, an area where tuberculosis is common. They enrolled healthy volunteers without signs of infection and newly diagnosed patients with lung tuberculosis confirmed by standard tests. Blood and fluid washed from the lungs, called bronchoalveolar lavage, were collected at the time of diagnosis and again at several points during the six-month course of therapy. All participants were HIV negative, which helped the team focus on tuberculosis itself rather than the effects of another major infection.
Two simple signs in the blood
The team focused on two main features in blood. The first was the monocyte to lymphocyte ratio, or MLR, which compares two common types of white blood cells that change during infection. The second was osteopontin, a protein involved in inflammation and tissue repair that circulates in the blood and is also present in the lungs. At the time of tuberculosis diagnosis, patients had a clearly higher MLR than healthy volunteers, and this pattern, together with other routine blood-count measures, separated the two groups in a statistical analysis. Plasma osteopontin levels were also higher in patients at diagnosis and again at the end of treatment compared with healthy controls, suggesting that both MLR and osteopontin are closely tied to active disease.
Signals from lung fluid and other immune messengers
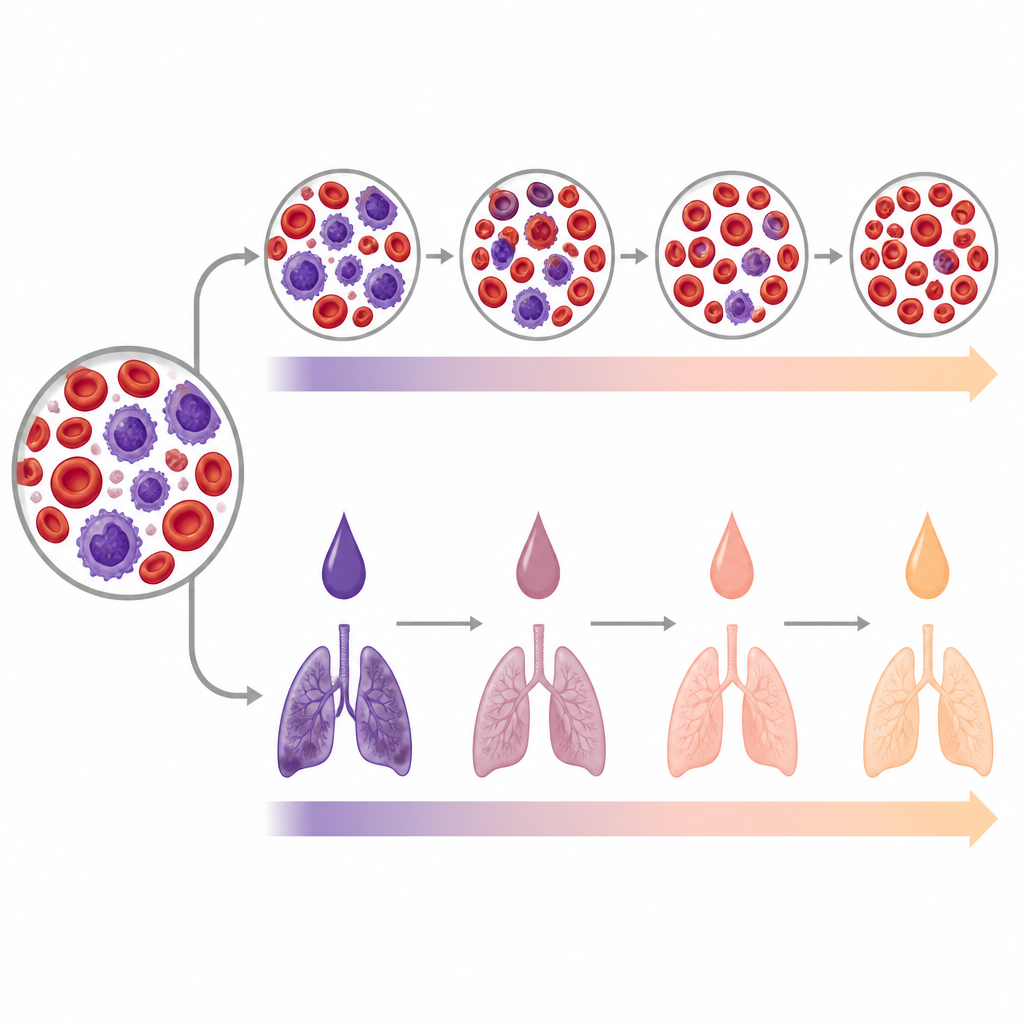
To see what was happening directly in the lungs, the scientists measured osteopontin and several inflammatory molecules in lung fluid. At diagnosis, osteopontin in this lung fluid did not differ much from healthy controls, but it rose by the end of treatment, even as plasma osteopontin showed no clear paired change between diagnosis and six months. This hints that osteopontin’s actions during tuberculosis might be more local to the lungs than in the whole bloodstream. Other immune messengers in plasma, including IL-6, VEGF-A, and sFasL, were high at diagnosis and tended to fall during treatment, especially in the first weeks and months, though some remained above control levels later. In lung fluid, IL-6 and TRAIL stayed elevated at both diagnosis and six months, while VEGF-A increased only modestly over time.
What the changing patterns may mean
These shifting patterns tell a story about how the body responds to tuberculosis and to the drugs used to treat it. High MLR at diagnosis fits with a picture of strong inflammation, with more monocytes and relatively fewer lymphocytes in the blood. The way osteopontin drops early in treatment but rises again by six months, especially in the lungs, suggests it may play a complex role in both damaging inflammation and healing. Routine blood tests also showed broader signs of inflammation in patients, such as higher white blood cell and platelet counts and lower hemoglobin, reinforcing the idea that active tuberculosis strongly reshapes the blood and immune system.
What this could mean for future TB care
The authors stress that their work is preliminary, based on modest numbers of patients and without groups such as people with latent infection or other lung diseases for comparison. Still, their findings point to the monocyte to lymphocyte ratio, osteopontin, and IL-6 as promising pieces of a future toolkit for tuberculosis monitoring. Because MLR comes from a standard full blood count and osteopontin can be measured from a simple blood sample, these markers could one day help clinicians in resource limited settings identify patients with active disease, track who is responding well to treatment, and decide who might need closer follow up after therapy ends.
Citation: Motaung, B., Holtzhausen, AR., Stanley, K. et al. The value of the monocyte-to-lymphocyte ratio and osteopontin (SPP1) in tuberculosis treatment response monitoring. Sci Rep 16, 15390 (2026). https://doi.org/10.1038/s41598-026-46176-8
Keywords: tuberculosis biomarkers, osteopontin, monocyte lymphocyte ratio, treatment monitoring, inflammation