Clear Sky Science · en
Anatomical characterization and visualization of the left dominant inferior mesenteric ganglionated plexus for nerve sparing colorectal surgery
Why Hidden Nerves Matter in Colon Surgery
Modern colon and rectal cancer surgery can save lives, but it sometimes leaves patients with lasting problems using the bathroom or with bladder and sexual function. This study looks closely at a small, easily overlooked group of nerves that wrap around a blood vessel deep in the abdomen. By mapping exactly where these nerves sit and how they vary from person to person, the researchers hope to help surgeons remove cancer while better preserving everyday bodily functions.
A Small Nerve Hub with a Big Job
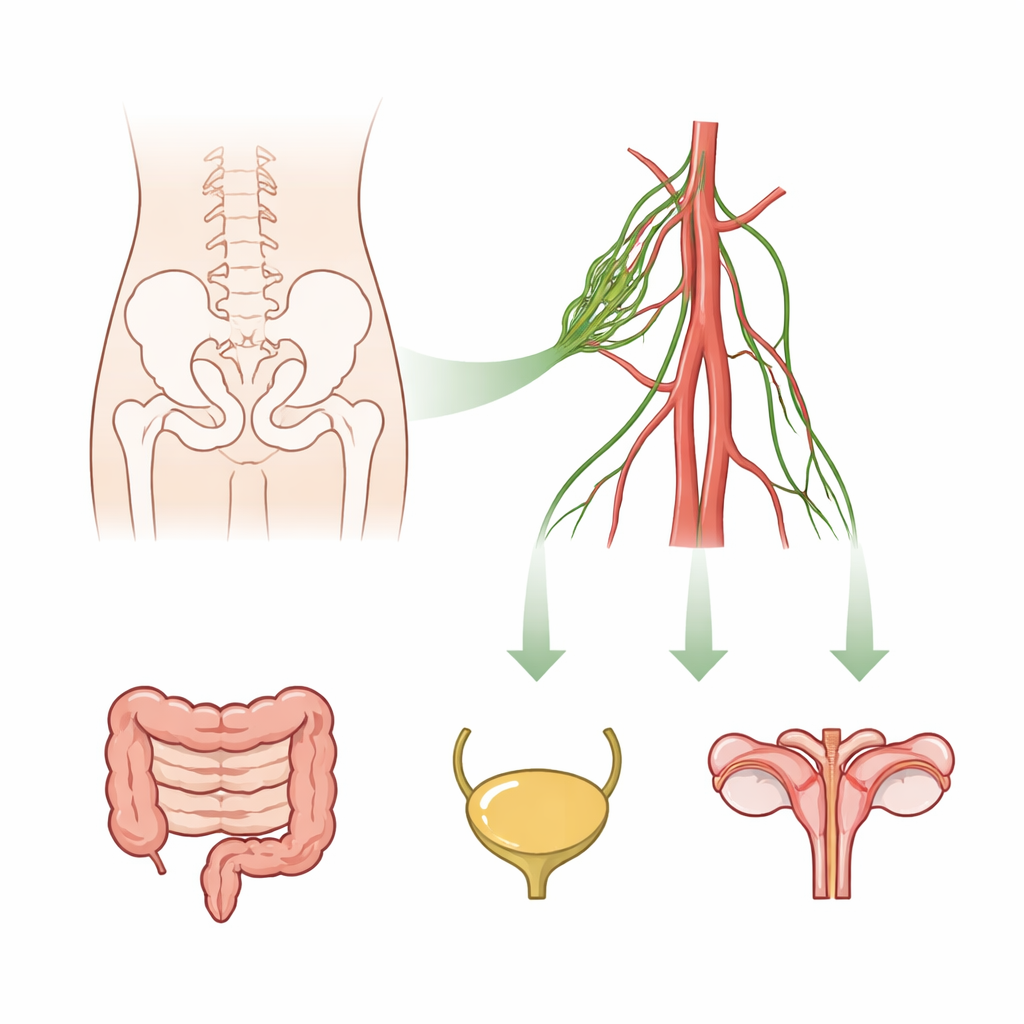
At the center of this work is a nerve web called the inferior mesenteric plexus, which helps control the lower part of the large intestine as well as nearby organs like the bladder and reproductive organs. Within this web are tiny swellings called ganglia, which act like relay stations for nerve signals. Animal experiments have long shown that a major ganglion in this region is crucial for bowel and pelvic organ control, but in humans this structure is small, hard to see, and inconsistently described in textbooks. As a result, surgeons have often treated the entire nerve area around the key blood vessel—the inferior mesenteric artery—as a vague tangle, rather than a structure with specific clusters that should be preserved.
Peering Closely at Donated Bodies
To bring clarity, the authors carefully dissected the relevant blood vessels and nerves in 17 donated human bodies and confirmed what they saw under the microscope. They found that, although less developed than in many laboratory animals, humans consistently possess small nerve ganglia associated with the artery that feeds the lower colon and rectum. These ganglia were not spread randomly. Instead, they tended to cluster on the left or left-back side of the artery, forming what the authors call a “left-dominant inferior mesenteric ganglionated plexus.” Because standard surgical and laparoscopic views usually look from the front or front-right, this left-sided cluster is often literally hidden from view during operations.
How Artery Shape Predicts Nerve Clusters
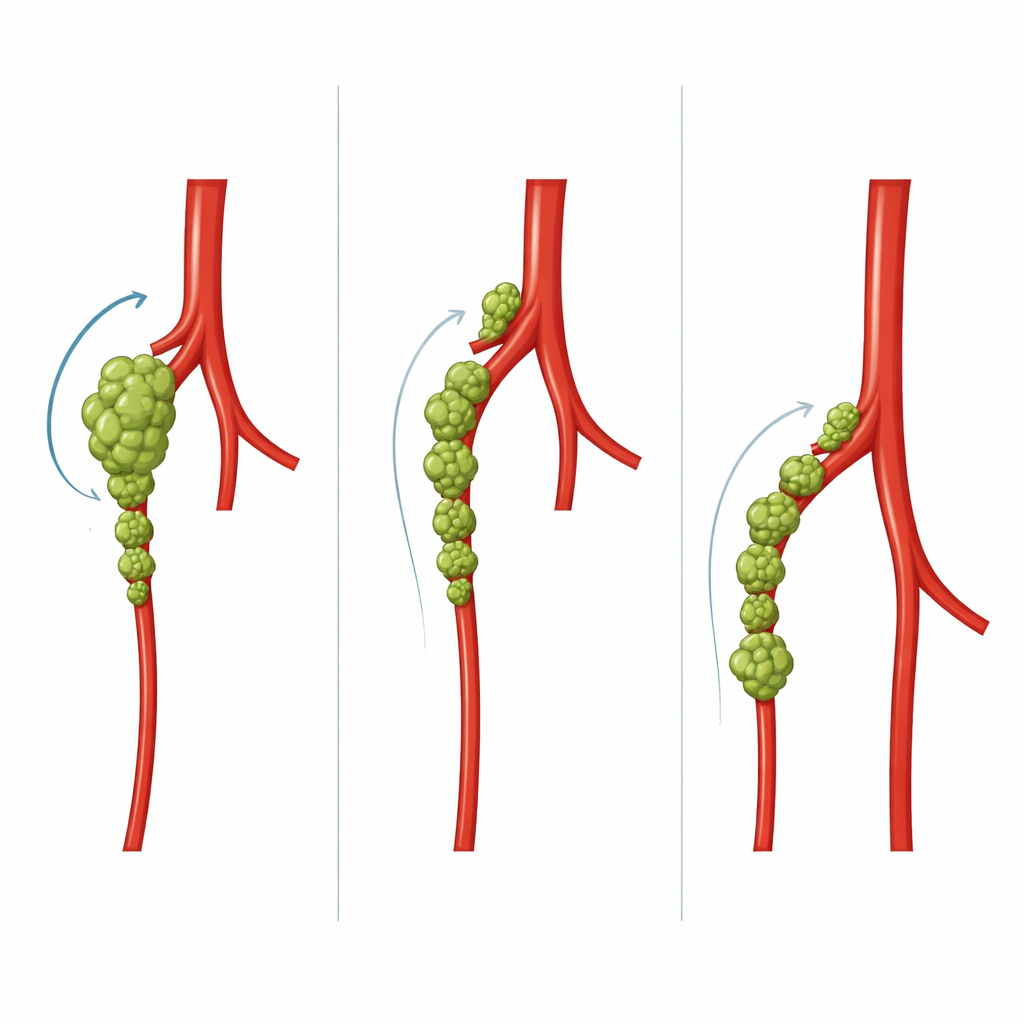
The team then examined how the branching pattern of the main artery related to the number and size of these nerve clusters. When the artery split early into a branch for the left side of the colon and the remaining trunk was short, there was typically one very large ganglion close to that early fork. When the artery trunk was longer and split farther down into several branches, the researchers saw several smaller ganglia lined up along the left side, with the largest usually sitting at the final branching point. In other words, the way the artery is shaped—its length and where it divides—strongly predicts where and how big these nerve clusters will be. Three-dimensional imaging models confirmed that these left-sided ganglia are difficult to spot from normal operative angles.
Lessons from Development and Evolution
The authors also compared their findings with what is known from animal studies and from how the digestive system develops before birth. In many common laboratory animals, a single, prominent ganglion often forms farther along the artery and hangs more freely in the abdomen. In humans and other primates, the layout is more complex: the ganglia are integrated into a broader nerve web at the root of the artery and tend to shift toward the left as the gut twists and settles into its adult position. This helps explain why the human version of this nerve hub is both more subtle and more asymmetrically placed than in experimental animals, making it harder to recognize without careful anatomical study.
What This Means for Patients
For people facing colorectal cancer surgery, the practical message is that preserving these small, left-sided nerve clusters may protect bowel, bladder, and sexual function after the operation. Because the size and location of the ganglia track closely with how the artery branches, surgeons could use preoperative imaging of the artery to predict where the nerves are most likely to be and adjust their dissection accordingly. When visual identification is still difficult—especially when lymph nodes are swollen by cancer—the authors suggest using special dyes or fluorescent markers to distinguish lymph tissue from nerve tissue. Overall, the study turns an obscure collection of tiny nerve knots into a clearly mapped target for safer, more function-preserving colorectal surgery.
Citation: Yaguchi, M., Kawashima, T. Anatomical characterization and visualization of the left dominant inferior mesenteric ganglionated plexus for nerve sparing colorectal surgery. Sci Rep 16, 11635 (2026). https://doi.org/10.1038/s41598-026-39814-8
Keywords: colorectal surgery, autonomic nerves, inferior mesenteric artery, nerve preservation, pelvic function