Clear Sky Science · en
CRISPR−Cas9 CD33-deleted allogeneic hematopoietic cell transplantation with gemtuzumab ozogamicin maintenance in AML: a phase 1/2 trial
Why this new approach matters
For adults with certain aggressive blood cancers, a donor stem cell transplant can be life saving but is often not the end of the story. Many patients still see their leukemia return, and some of the drugs that best attack cancer cells also damage the new healthy blood system. This study explores a way to genetically tweak donor stem cells so they can better tolerate a powerful targeted drug, opening the door to longer lasting protection against relapse.
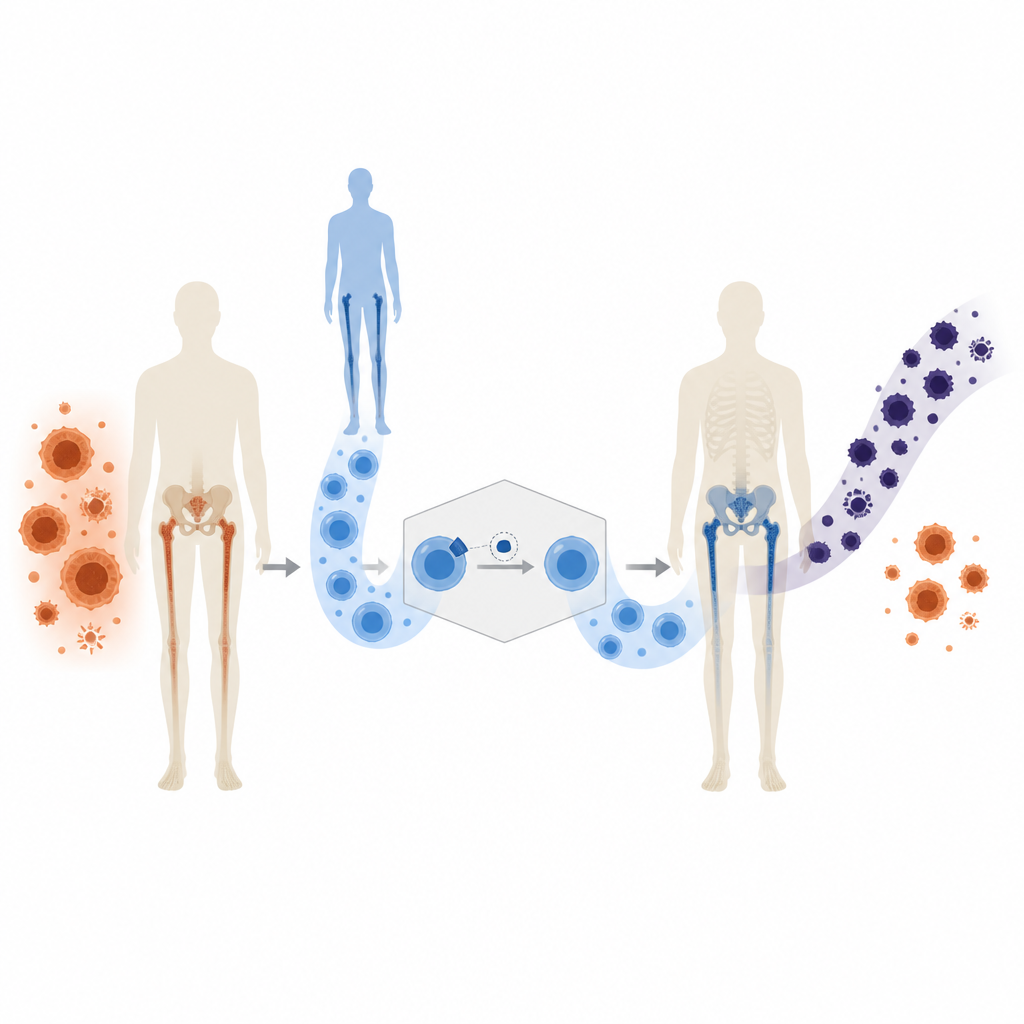
Turning a shared target into a cancer specific one
Many leukemia cells display a marker called CD33 on their surface, which makes them vulnerable to a drug called gemtuzumab ozogamicin, a type of targeted chemotherapy. The problem is that normal blood forming cells also carry CD33, so the drug can wipe out healthy cells along with cancer. The researchers tested a transplant product nicknamed trem cel, in which donor stem and progenitor cells were edited with CRISPR so they no longer make CD33. The idea is simple: remove CD33 from the incoming healthy cells so that, after the transplant, doctors can safely give a CD33 seeking drug that mainly sees cancer cells.
Testing the edited transplant in real patients
The phase 1/2a trial enrolled 30 adults with acute myeloid leukemia or a related bone marrow disorder who were at especially high risk of their disease returning after transplant. All patients received intensive chemotherapy or radiation, followed by the trem cel transplant from a closely matched donor. Around two months later, if their blood counts had recovered and their disease was under control, they began regular low dose infusions of gemtuzumab ozogamicin once every four weeks, for up to eight cycles. Nineteen patients started this maintenance treatment while others were still too early, had relapsed, or were not eligible.
How the edited cells behaved in the body
Every one of the 30 patients who got trem cel reached the main safety goal: their white blood cell counts recovered within 28 days, with a typical recovery time of about ten days. Platelet counts also came back at speeds similar to standard unedited transplants. Detailed blood tests showed that donor cells took over the production of key immune cell types and that the CD33 deletion remained stable across myeloid, B cell, T cell and natural killer cell lineages. Importantly, the loss of CD33 did not measurably weaken basic neutrophil function or the rebuilding of a diverse immune system, suggesting that the edit did not handicap normal blood formation.
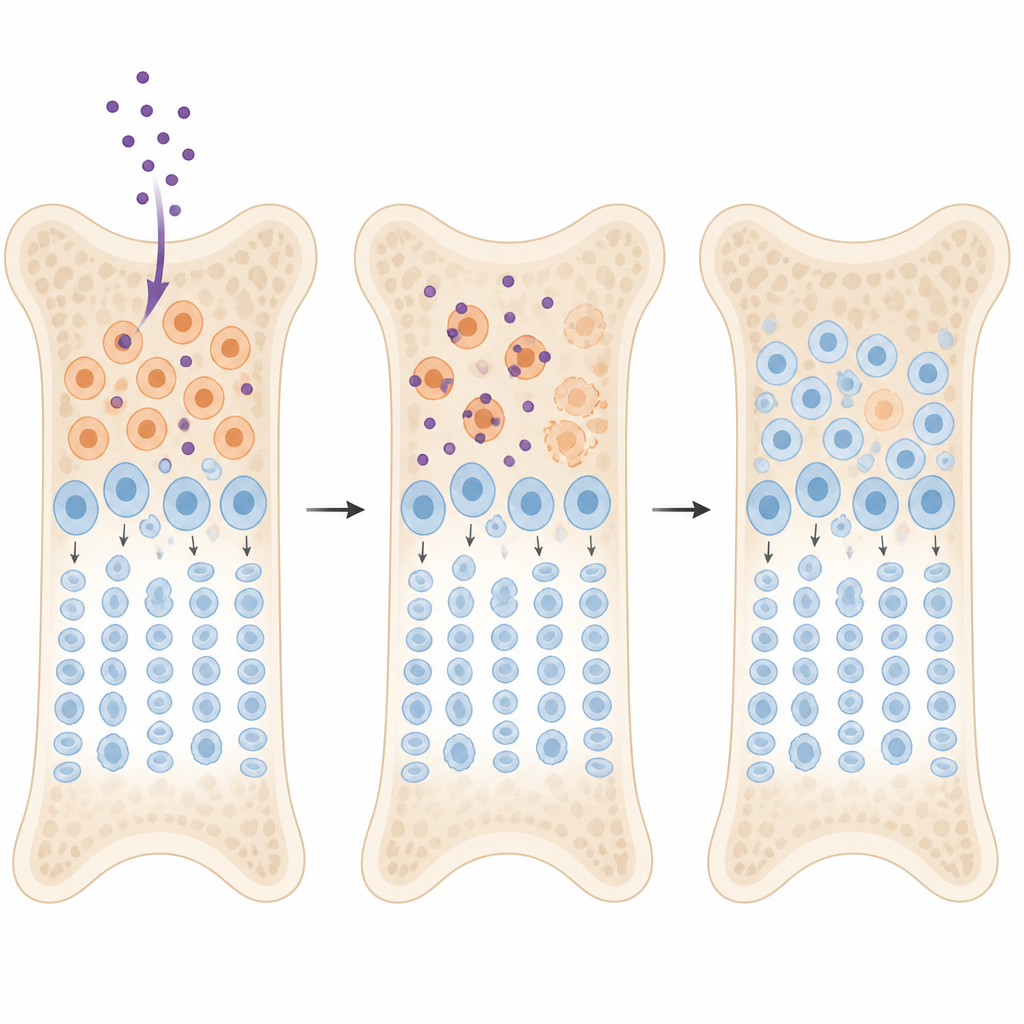
Using an old drug in a new way
When gemtuzumab ozogamicin was added after transplant, patients generally tolerated it well up to the recommended phase 2 dose of 2 milligrams per square meter given once per 28 day cycle. Blood counts stayed largely steady without the long lasting severe drops that usually limit this drug after a standard transplant. One serious liver related complication linked to the drug occurred months after dosing in a patient with several other medical stresses. Drug level measurements showed that in the CD33 negative setting, gemtuzumab ozogamicin stayed in the body longer but did not reach sharply higher peak levels, hinting at a wider safety window while still engaging remaining CD33 positive cells.
What this could mean for patients
Although the trial was small and follow up time was modest, patients had a relapse free survival of about 14 months and roughly two in five were free of relapse at around two years, encouraging numbers in such a high risk group. All relapses that did occur still showed CD33 on leukemia cells, implying that resistance arose through pathways other than simply losing the target. To a lay reader, the take home message is that editing donor stem cells so they lack CD33 allowed doctors to give a targeted anti CD33 drug after transplant without the usual, prolonged damage to healthy blood cells. This early proof of principle suggests that shielding the transplant in this way could make maintenance treatment safer and more effective, and similar strategies might be applied to other targets in the future.
Citation: DiPersio, J.F., Koehne, G., Shah, N.N. et al. CRISPR−Cas9 CD33-deleted allogeneic hematopoietic cell transplantation with gemtuzumab ozogamicin maintenance in AML: a phase 1/2 trial. Nat Med 32, 1763–1772 (2026). https://doi.org/10.1038/s41591-026-04362-1
Keywords: acute myeloid leukemia, stem cell transplant, CRISPR gene editing, targeted chemotherapy, immunotherapy maintenance