Clear Sky Science · en
Pembrolizumab and olaparib in homologous-recombination-deficient metastatic pancreatic cancer: the phase 2 POLAR trial
Why this study matters for patients and families
Pancreatic cancer is often discovered late and has been very hard to treat, with most patients living only a short time after diagnosis. This study explores whether a smart maintenance treatment, given after initial chemotherapy has worked, can keep the cancer in check longer for people whose tumors carry certain inherited or acquired DNA repair glitches. It asks a hopeful question: can pairing a targeted pill with an immune therapy, and choosing patients by their tumor genetics, turn a short-lived response into longer control for some?
Building on early wins from genetics and immune therapy
Doctors already know that a small share of people with pancreatic cancer have changes in genes such as BRCA1, BRCA2 or PALB2 that weaken the tumor’s ability to repair broken DNA. These tumors tend to respond well to platinum chemotherapy and to a drug class called PARP inhibitors, which take further advantage of this weakness. Separately, immune checkpoint drugs that wake up the body’s T cells have helped a tiny subset of patients whose tumors have a high number of mutations. The POLAR trial set out to combine these ideas: use platinum chemotherapy first to shrink the cancer, then switch to a maintenance mix of the PARP blocker olaparib and the immune drug pembrolizumab, focusing on patients most likely to benefit based on their genes and chemotherapy response. 
Three patient groups with different genetic stories
The trial enrolled 63 people with metastatic pancreatic cancer at a single cancer center and sorted them into three groups. Cohort A included 33 patients whose tumors had the well-known DNA repair changes in BRCA1, BRCA2 or PALB2. Cohort B included 15 patients with changes in other DNA repair genes that might act in a similar way. Cohort C included 15 patients without these repair gene changes but whose cancers had stayed sensitive to platinum chemotherapy for at least six months. Everyone had completed several months of platinum treatment without tumor growth, then started maintenance olaparib tablets and pembrolizumab infusions, continuing as long as the cancer stayed controlled and side effects were manageable.
How well the maintenance approach worked
The main yardsticks were how many patients had further measurable tumor shrinkage and how many were free of progression six months into maintenance. In the BRCA1/BRCA2/PALB2 group, about one in three patients with measurable tumors saw additional shrinkage, and almost two in three were still progression free at six months. These numbers fell short of the ambitious goals the team had set in advance, but longer follow-up told a more encouraging story: half of these patients were alive at just over two years, and nearly half were still alive at three years, which compares favorably with past trials using olaparib alone. The other two groups, without the core gene changes, saw fewer responses and shorter periods before the cancer grew again, suggesting that the maintenance mix is most helpful in the clearly DNA repair–defective group.
Clues from blood and tissue about who benefits
Because not all patients in the main genetic group did equally well, the researchers dug deeper into blood and tumor samples. They tracked fragments of tumor DNA in the bloodstream and found that patients whose blood showed little or no detectable tumor DNA during maintenance were more likely to enjoy long control of their disease. Detailed sequencing of tumor samples showed that cancers with broken DNA repair had more of a certain kind of mutation that can create unusual protein fragments, which the immune system can recognize. These tumors also tended to have more immune cells, especially T cells, sitting in and around them, and higher levels of these immune visitors were linked to longer benefit. 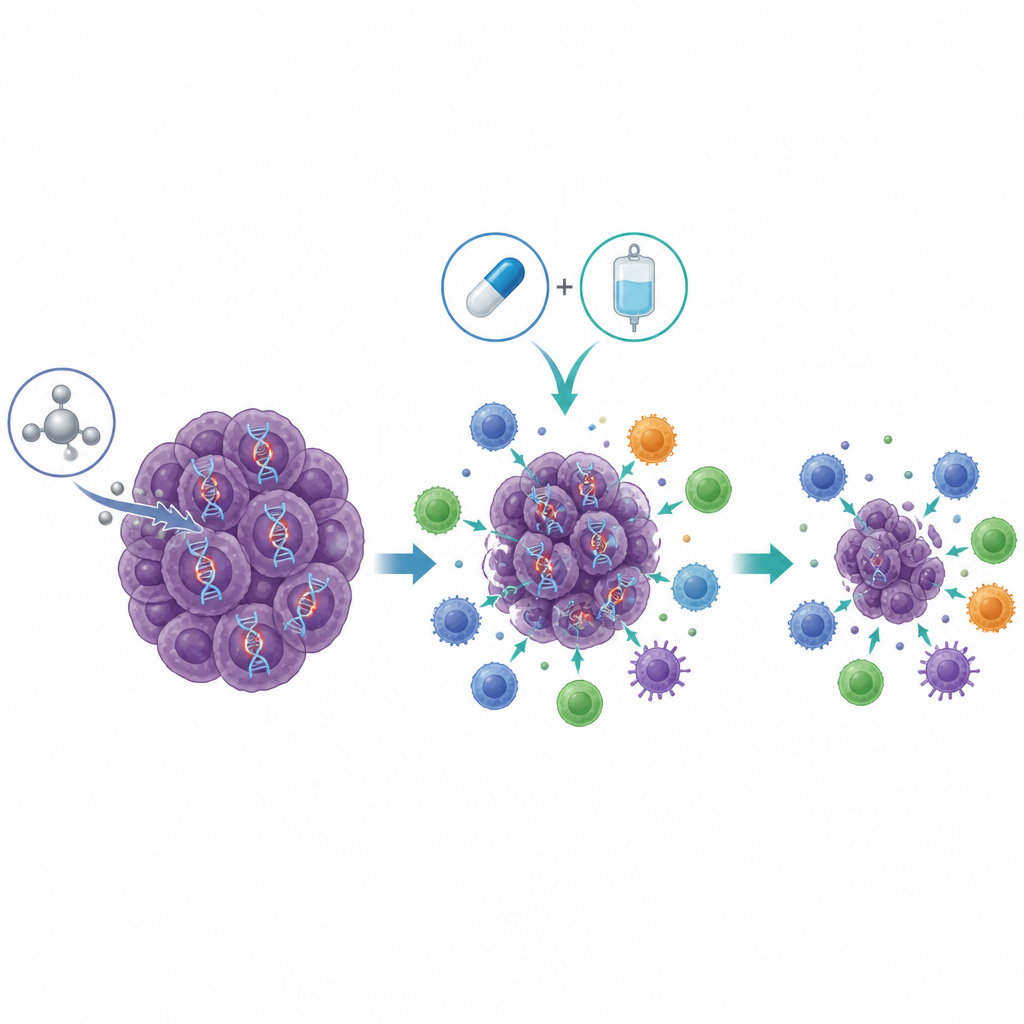
What this could mean for future care
Taken together, the results suggest that while this maintenance combination is not a cure, it can bring years of added life to a meaningful subset of people whose pancreatic tumors have specific DNA repair defects and who respond well to platinum chemotherapy. The work supports a model in which damaged tumor DNA creates signals that can attract immune attack, and the drug combination both exploits the DNA weakness and boosts immune pressure. The study strengthens the case for routine genetic testing in pancreatic cancer, for monitoring tumor DNA in blood as a marker of deep response, and for larger trials that fine-tune which patients should receive this kind of precision maintenance treatment.
Citation: Park, W., O’Connor, C.A., Chou, J.F. et al. Pembrolizumab and olaparib in homologous-recombination-deficient metastatic pancreatic cancer: the phase 2 POLAR trial. Nat Med 32, 1783–1793 (2026). https://doi.org/10.1038/s41591-026-04299-5
Keywords: pancreatic cancer, pembrolizumab, olaparib, BRCA mutations, precision immunotherapy