Clear Sky Science · en
Bispecific GLP-1/GLP-2 agonism in advanced type 2 diabetes: preclinical characterization and a randomized, double-blind, placebo-controlled phase I trial
Why this new diabetes drug approach matters
People with advanced type 2 diabetes often face a harsh trade-off: strong medicines can lower blood sugar but may also cause stomach distress and further weight loss in patients who are already losing muscle and fat. This study introduces PG-102, an experimental drug designed to control blood sugar while helping the body keep its weight and strength, offering hope for those who do not fit the typical “weight loss is good” picture in diabetes care.
A two-in-one signal for gut and pancreas
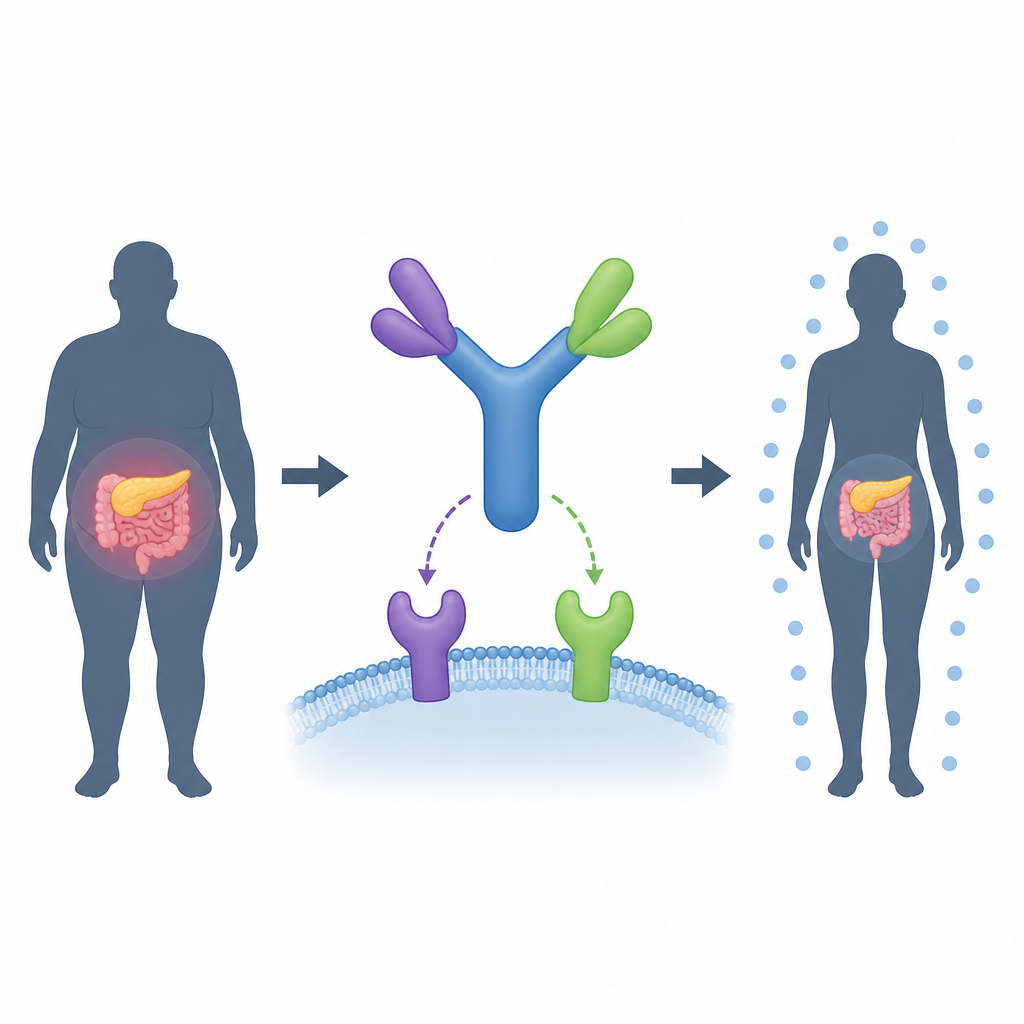
PG-102 is built to activate two natural hormone signals at once, called GLP-1 and GLP-2. GLP-1 based drugs are now standard treatments because they lower blood sugar, reduce appetite, and protect the heart and kidneys. But they can cause nausea and unwanted weight loss, and many patients still do not reach their blood sugar goals. GLP-2, in contrast, is better known for helping the gut repair itself, and it also supports insulin-producing cells and improves how tissues use sugar without strongly pushing the body to release more insulin. PG-102 fuses GLP-1 and GLP-2 actions into a single long-lasting antibody-like molecule whose design carefully tones down GLP-2 activity to avoid over-growth of the intestine while keeping its helpful effects.
Stronger blood sugar control without extra wasting in mice
The researchers first tested PG-102 in db/db mice, a well-established model of severe type 2 diabetes in which animals have very high blood sugar, failing insulin-producing cells, and marked weight loss. Over three months, PG-102 lowered blood sugar and long-term glucose markers much more than two leading drugs, semaglutide and tirzepatide. Many PG-102 treated mice achieved near-normal sugar levels and kept them stable, whereas the other drugs lost effect over time. Under the microscope, PG-102 preserved the size and structure of the pancreatic islets, maintained the number of insulin-producing beta cells, and reduced markers of local inflammation compared with untreated animals and with the comparator drugs.
How the dual action helps cells handle sugar
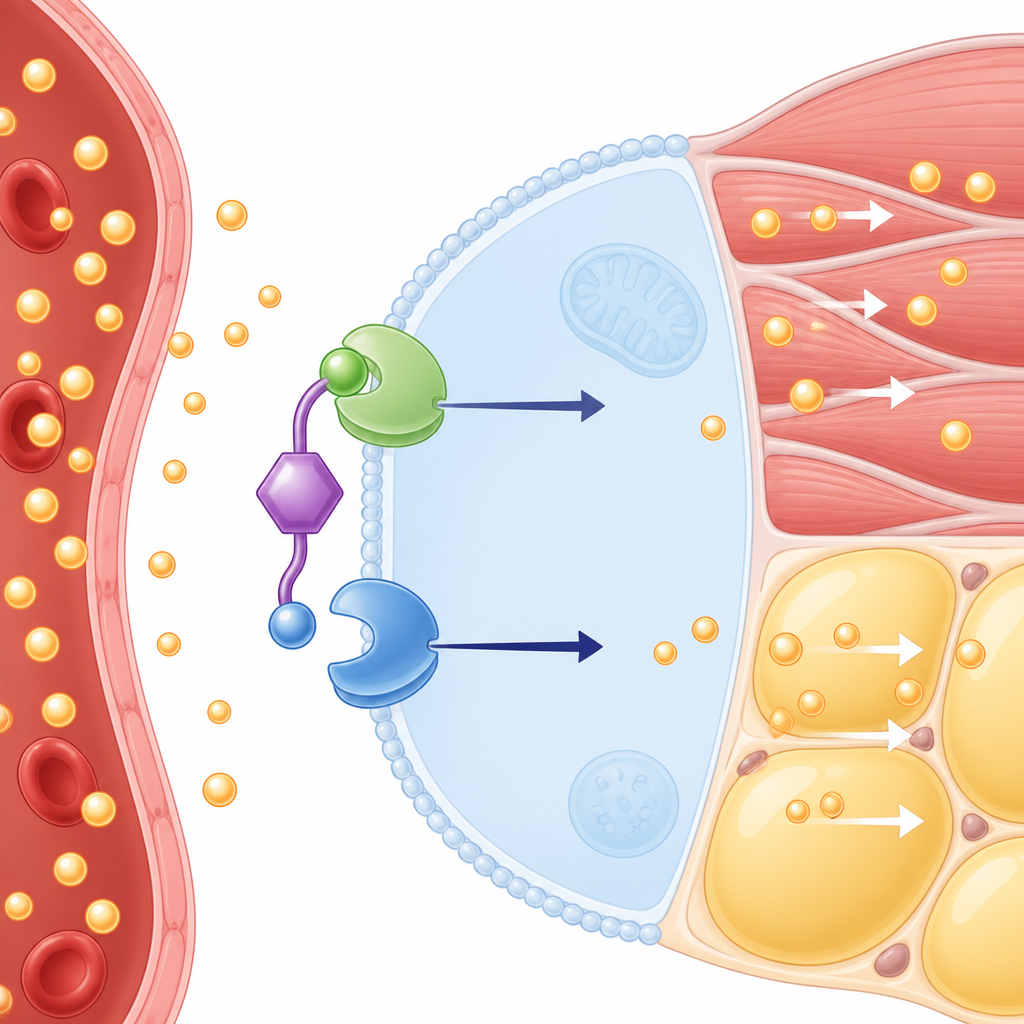
To understand how PG-102 works, the team studied isolated cells and tissues. In pancreas-like cell lines, PG-102 better protected cells from a toxic stress that mimics diabetes and supported their ability to release insulin when exposed to high glucose. It boosted key genes that maintain beta cell identity and function. In fat cells and muscle-like cells, PG-102 increased the uptake of a glucose tracer more than either single-hormone version or their combination given separately, pointing to a true synergy of the two signals on the same cell. Blocking GLP-2 receptors largely removed this effect, suggesting that even a modest GLP-2 signal can strongly drive sugar entry into tissues when linked to GLP-1 in one molecule. Imaging studies further showed that PG-102 changes how the two receptors move on the cell surface, keeping them active together for longer.
Decoupling sugar control from weight loss
A striking feature of PG-102 in the mouse studies was its ability to separate blood sugar control from further weight loss. In advanced disease, untreated mice lost up to 40% of their body weight, reflecting severe breakdown of muscle and fat. PG-102 not only normalized blood sugar but also largely prevented this wasting, whereas semaglutide and tirzepatide allowed or added to weight loss. The authors suggest that PG-102 restores more normal fuel use, reduces the need to burn muscle and fat, may tap into GLP-2 linked pathways that protect muscle proteins, and improves gut barrier function in ways that dampen chronic inflammation, all of which can support body mass instead of eroding it.
Early human trial shows acceptable safety
The team then carried out a first-in-human multiple dose trial in 24 adults with overweight but without diabetes. Participants received several weekly injections of PG-102 at different doses or placebo. The main goal was safety, and PG-102 was generally well tolerated: most side effects were mild digestive issues such as indigestion, nausea, and diarrhea, at rates similar to or only slightly higher than placebo, and no serious events occurred. Blood measurements showed a long half-life of about four to five days and dose-proportional exposure, suggesting that weekly dosing should be feasible. In an oral sugar challenge at the end of treatment, those given PG-102 cleared sugar from the blood faster and had lower overall sugar exposure than those given placebo, hinting at meaningful metabolic activity even in this short study.
What this could mean for people with advanced diabetes
The findings suggest that combining GLP-1 and GLP-2 actions in a single, carefully tuned drug can deliver stronger and more durable blood sugar control in severe diabetes models while preserving body weight and limiting stomach-related side effects in early human testing. For patients with advanced type 2 diabetes who are already losing weight and muscle, PG-102 or similar drugs could one day offer sugar control without further frailty, though larger and longer clinical trials in people with diabetes are still needed to confirm these benefits.
Citation: Yang, SI., Kim, S.W., Son, KH. et al. Bispecific GLP-1/GLP-2 agonism in advanced type 2 diabetes: preclinical characterization and a randomized, double-blind, placebo-controlled phase I trial. Nat Commun 17, 4477 (2026). https://doi.org/10.1038/s41467-026-71080-0
Keywords: type 2 diabetes, GLP-1, GLP-2, incretin therapy, beta cell protection