Clear Sky Science · en
Feasibility and reproducibility of handheld and table-mounted optical coherence tomography in children with craniosynostosis
Why this matters for children’s sight
When the bones of a baby’s skull fuse too early, the pressure inside the head can rise and threaten the child’s eyesight. Doctors need safe, simple ways to keep watch on the nerve at the back of the eye, which can show early signs of this pressure. This study asked whether a small handheld eye scanner gives results that match a larger table-mounted scanner, so that children can be monitored more easily in clinics and hospitals.
Two ways to take a picture of the eye
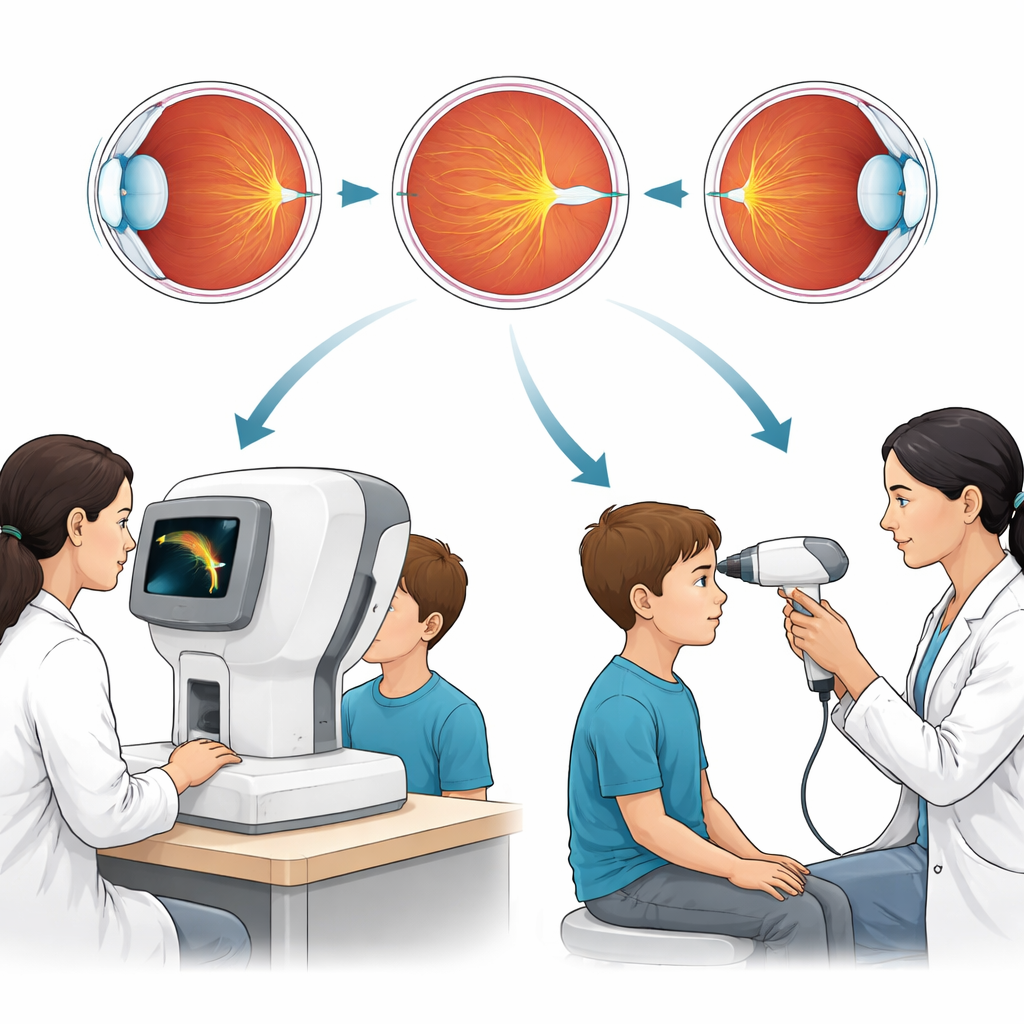
The researchers focused on a technology called optical coherence tomography, or OCT, which uses light to create detailed cross section pictures of the back of the eye. One version is a large unit where the child rests their chin and looks into the machine, while the other is a lightweight handheld scanner that can be brought to the child. Because children with craniosynostosis often need repeated checks, being able to use either machine confidently could make eye care more flexible and less stressful.
Who took part in the study
The team worked with twenty children aged between four and sixteen years who had craniosynostosis, a condition where skull bones fuse too early. Some had a known genetic syndrome, while others did not. All were seen at a specialist children’s hospital. Each child had both eyes scanned first with the table-mounted Spectralis machine and then with the handheld Envisu device in the same visit, so the images could be compared directly.
How the scans were compared
From each scan, the researchers measured several features of the optic nerve, such as the size and depth of the central hollow and the thickness of the surrounding nerve tissue. These details can reveal swelling from raised pressure or thinning from damage. They then used statistical tests to see how closely the numbers from the two machines matched and how much they varied. They also asked an expert and a newly trained grader to judge visual signs of pressure on the scans without knowing which machine produced them.
What the researchers found
Every child completed successful scans on both machines, showing that even school aged children can manage the more traditional table unit as well as the handheld device. For nearly all measured features of the optic nerve, the two machines gave results that agreed very closely, with only small differences that are unlikely to matter in day to day care. The visual judgments of pressure related changes were almost identical between machines and between graders, especially after brief training, suggesting that doctors and technicians can learn to read these scans consistently.
What this means for families and clinicians
The study suggests that handheld and table mounted OCT scanners can be used side by side to monitor the optic nerve in children with craniosynostosis. In practical terms, this means that a child scanned with a handheld device when very young can later be scanned on a table unit, and their results can still be compared with confidence. It also means that data from both types of machines can be combined in research studies, helping doctors refine how they detect harmful pressure early and protect children’s sight over time.
Citation: Rufai, S.R., Roche, D., Shenoy, R. et al. Feasibility and reproducibility of handheld and table-mounted optical coherence tomography in children with craniosynostosis. Eye 40, 1043–1049 (2026). https://doi.org/10.1038/s41433-026-04317-3
Keywords: craniosynostosis, optic nerve imaging, handheld OCT, pediatric ophthalmology, intracranial pressure