Clear Sky Science · en
CSF1R inhibitors mitigate CDK4/6 inhibitor-induced immunosuppression to increase antitumor immunity in HR+/HER2− breast cancer
Why this breast cancer study matters
Many women with common hormone-driven breast cancer respond poorly to current drug and immune treatments. This study asks why a widely used targeted drug can quietly weaken the body’s own defenses, and whether adding a second medicine can restore the immune system’s ability to attack the tumor.
A closer look at a common breast cancer type
The research focuses on breast cancers that are hormone receptor positive and lack the HER2 marker, a group that makes up about 70% of cases. These tumors often do not fully shrink with drug treatment before surgery, and survival after spread to distant organs remains unsatisfactory. Immune checkpoint drugs, which have helped other cancers, work less well here because these tumors tend to be filled with cells that dampen immune attack rather than with aggressive, tumor-fighting lymphocytes.
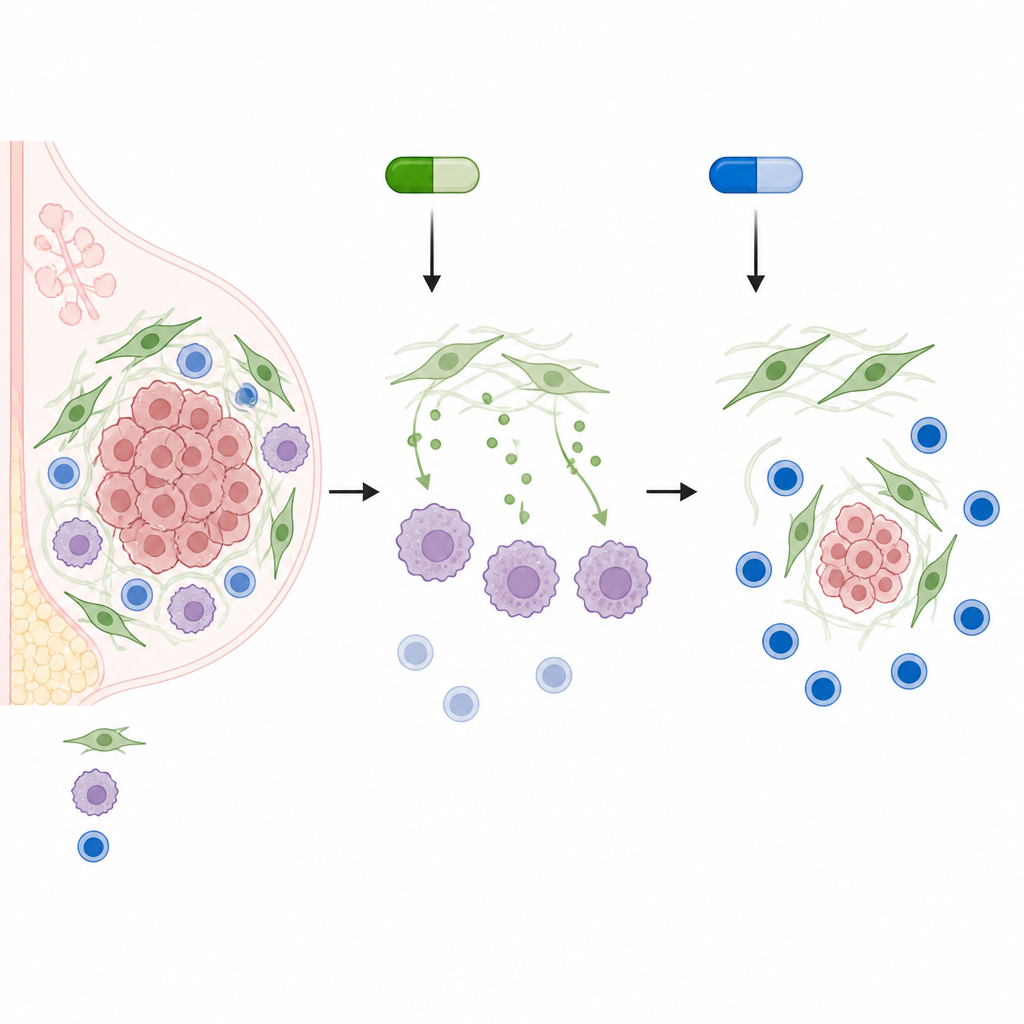
When a growth blocker turns the neighborhood quiet
Doctors often use CDK4/6 inhibitors such as palbociclib to slow tumor cell division in this breast cancer subtype. Using mouse tumors, patient samples, and mini-tumors grown in the lab, the authors discovered an unwanted side effect in the tumor neighborhood. Palbociclib pushed support cells called fibroblasts into a state similar to aging. In this state they released higher levels of two growth signals, IGF1 and FGF7. These signals reprogrammed nearby immune cells called macrophages into a nurturing, wound-healing mode that favors the tumor instead of fighting it. The reprogrammed macrophages produced large amounts of an enzyme, ARG1, which consumes the nutrient arginine that nearby T cells and natural killer cells need to stay active and multiply.
How immune cells are stalled rather than strengthened
Single-cell gene readouts and tissue imaging showed that palbociclib-treated tumors did not lose T cells in number, but these cells divided less and bore signs of fatigue. Communication networks between macrophages and lymphocytes, normally needed to switch on strong attack programs, were weakened. Inside macrophages, the fibroblast signals activated a switch called STAT3 at a specific site, Tyr705, which drove ARG1 production. The result was a chemically calm, suppressive environment: nutrient-starved T cells with low growth marker Ki-67, exhausted killer T cells expressing brakes such as PD-1 and TIM-3, and regulatory T cells that still carried strong suppression markers.
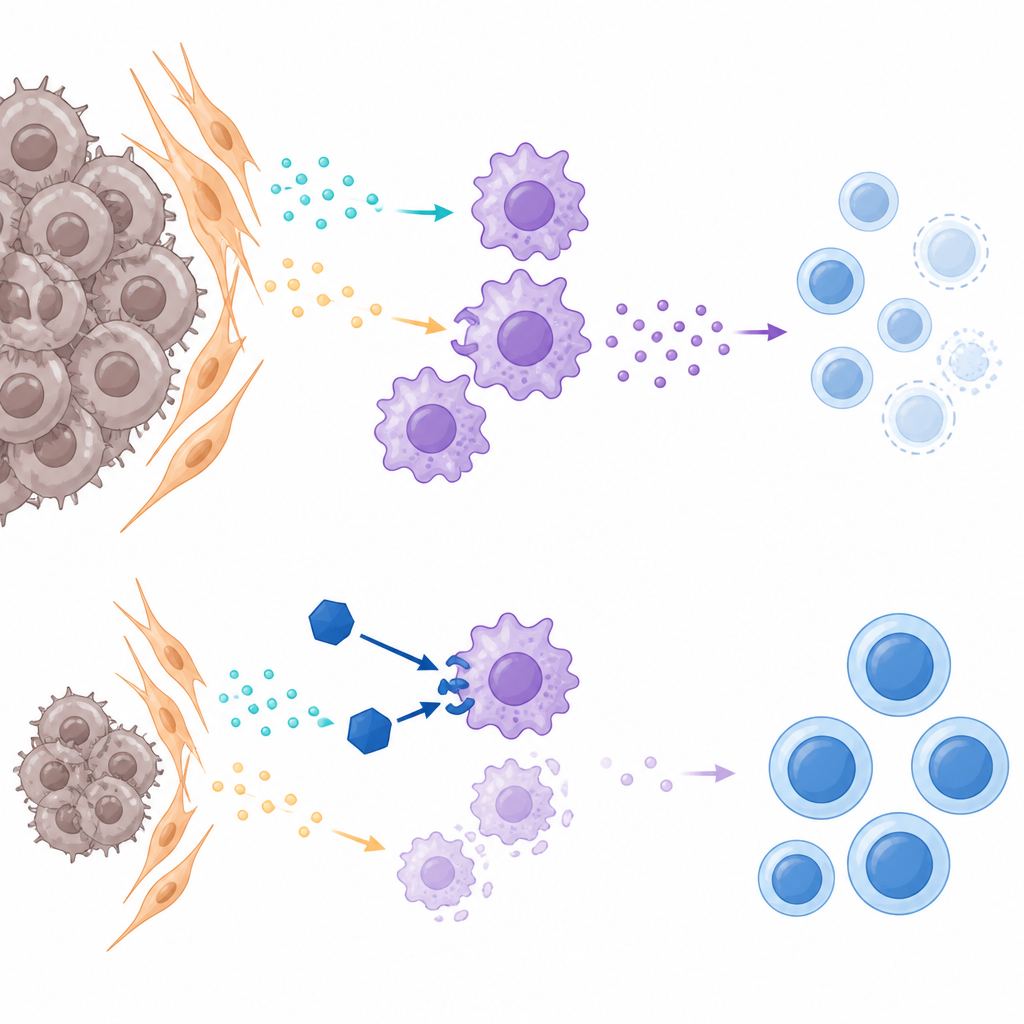
A second drug that lifts the immune brake
The team then tested drugs that directly target macrophages. They compared a CCR2 blocker, which mainly stops macrophage entry, with pexidartinib, a pill that blocks the CSF1R switch required for macrophage survival and function. In mouse tumors, pairing palbociclib with pexidartinib shrank tumors more than palbociclib alone, whereas the CCR2 blocker added little benefit. Pexidartinib reduced the number of macrophages, especially the ARG1-rich, tumor-helping type, restored arginine levels, and increased the presence and activity of CD4 and CD8 T cells and natural killer cells. Markers of T cell exhaustion fell, and regulatory T cells lost some of their strongest suppression signals.
Testing the combination on patient-derived mini-tumors
To bring the work closer to the clinic, the researchers grew three-dimensional organoids from untreated patient tumors and cocultured them with blood immune cells. In this setting, either palbociclib or pexidartinib alone slowed organoid growth, but the combination led to a clear drop in organoid size and number and reduced signs of cell health. These findings suggest that tackling both cancer cell division and the tumor’s protective immune cloak at once may produce stronger and more durable control.
What this could mean for patients
In simple terms, the study shows that a popular growth-blocking drug can unintentionally lull immune cells inside the tumor by reshaping nearby support and guardian cells. Adding a macrophage-blocking drug appears to undo much of this immune quieting, allowing T cells and natural killer cells to recover and join the fight against the cancer. While more testing is needed to confirm safety and benefit in people, the work points toward combination treatments that pair CDK4/6 inhibitors with CSF1R blockers to make hormone-driven, HER2-negative breast cancers more vulnerable to the body’s own defenses and possibly to future immunotherapy.
Citation: Li, S., Gong, Y., Li, H. et al. CSF1R inhibitors mitigate CDK4/6 inhibitor-induced immunosuppression to increase antitumor immunity in HR+/HER2− breast cancer. Oncogene 45, 1970–1987 (2026). https://doi.org/10.1038/s41388-026-03786-w
Keywords: HR positive breast cancer, CDK4/6 inhibitor, tumor immune microenvironment, macrophages, CSF1R inhibitor