Clear Sky Science · en
Preclinical evidence of sonodynamic therapy in glioblastoma and challenges towards clinical translation: a review of the literature
A new way to attack stubborn brain tumors
Glioblastoma is one of the deadliest brain cancers, and current treatments often buy patients only a little extra time. This article explores sonodynamic therapy, a noninvasive strategy that uses sound waves plus a drug that collects in tumor cells to damage cancer from within. For readers, it offers a look at how physics, chemistry, and medicine might join forces to tackle tumors that surgery, radiation, and chemotherapy still struggle to control.
How sound and a smart drug team up
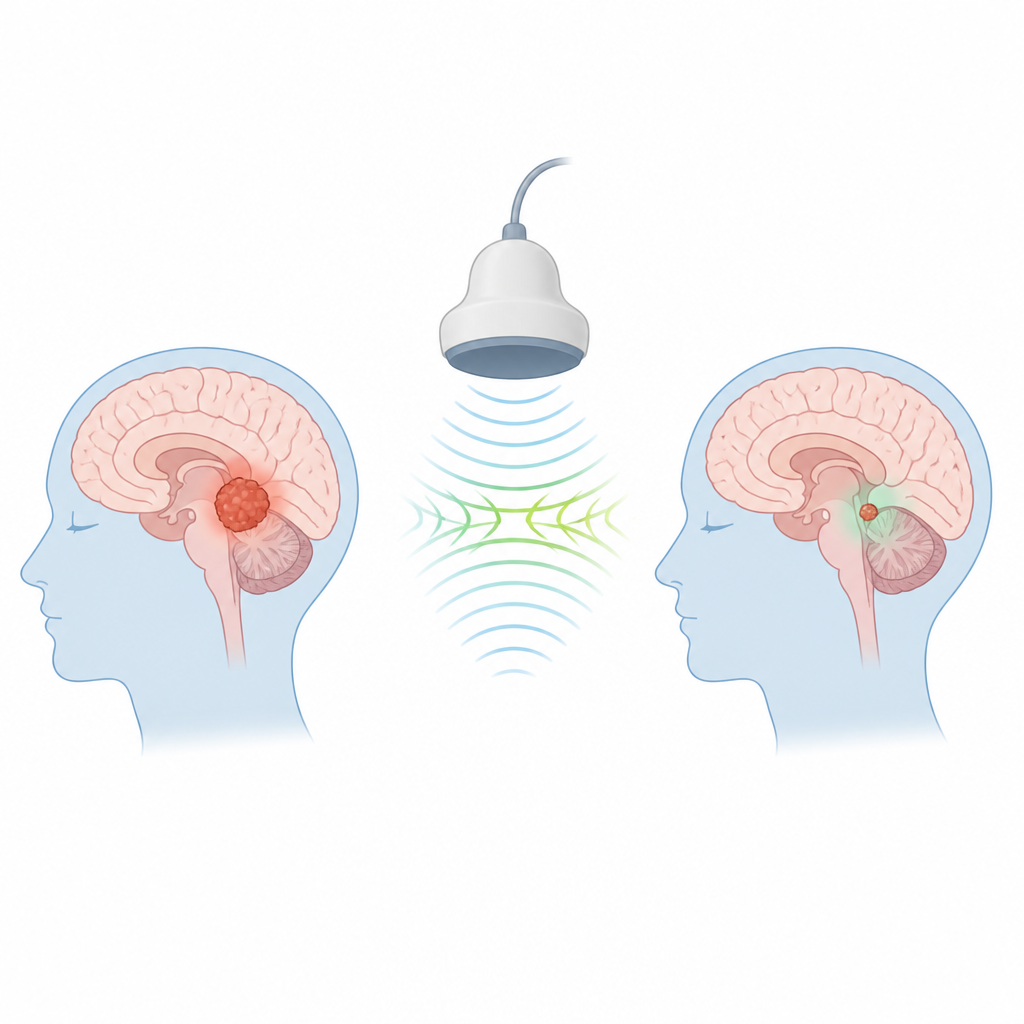
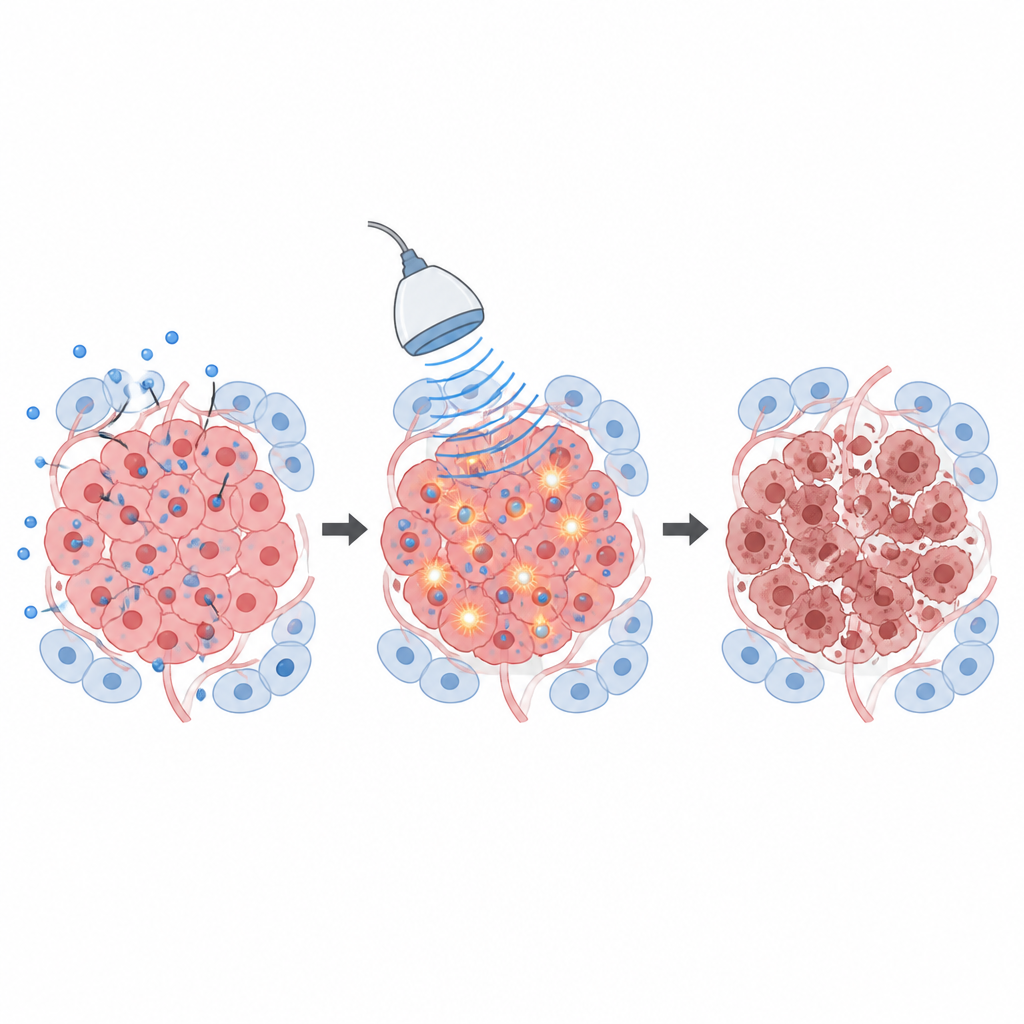
Sonodynamic therapy pairs focused ultrasound with a chemical known as a sonosensitizer. On its own, the drug is given at doses that are considered safe, and the ultrasound levels are also below those used to heat or burn tissue. The key is that the drug tends to build up more in tumor cells than in healthy brain, thanks to the leaky blood vessels and altered metabolism of cancer. When ultrasound is applied to the tumor region, it energizes the drug in the presence of oxygen, sparking the formation of short‑lived, highly reactive molecules that damage cell membranes, proteins, and DNA right where the drug has collected.
What happens inside targeted cancer cells
Once these reactive molecules are formed, they set off several kinds of cell death. Mitochondria, the cell’s power stations, can be injured so badly that they trigger programmed self‑destruction pathways, a neat and tidy form of death called apoptosis. If the damage is more severe, cells can swell and burst in an uncontrolled way, known as necrosis, which spills their contents into the surrounding tissue. This messy death can attract immune cells and may help the body recognize the tumor as a threat. Early work also suggests that sonodynamic therapy can stir up other regulated death routes and stress responses, hinting that its biological effects extend well beyond a simple “on–off” kill switch.
Fine‑tuning the sound and the drug
The review shows that how the sound is delivered matters greatly. Lower ultrasound frequencies travel deeper into the brain and make it easier to form and collapse tiny bubbles in tissue fluid, a process called cavitation that boosts the chemical reactions. Intensity, pulse pattern, and total exposure time must be balanced so that bubble activity is strong enough to damage tumor cells but not so strong that it overheats or tears healthy brain. In animal studies, most groups used low to moderate intensities and found that many different settings slowed tumor growth, yet they reported their methods in very different ways, which makes direct comparison difficult. Likewise, researchers tested several sonosensitizing drugs, with 5‑aminolevulinic acid, already used to make brain tumors glow during surgery, emerging as the most practical candidate for patients.
From animal studies to patient trials
The authors examined 13 preclinical studies in rodents and one safety study in pigs. Across these experiments, pairing a sonosensitizer with focused ultrasound repeatedly shrank tumors, reduced markers of cell division, increased signs of cell death, and, in many cases, prolonged survival. One study also found changes in immune cells that suggest the treatment might help the body mount a stronger attack on the tumor. However, nearly all of the animal work used different drug doses, timing, ultrasound machines, and measurement tools, and negative results were rarely reported. On the clinical side, six early‑phase trials in people with newly diagnosed or recurrent glioblastoma are under way or completed, almost all centered on 5‑aminolevulinic acid and low‑intensity ultrasound. These studies focus mainly on safety, short‑term tissue effects, and how well patients tolerate repeated treatments.
Barriers on the road to routine care
Despite encouraging signs, the article stresses that sonodynamic therapy is still far from routine clinical use. Researchers do not yet agree on the best ultrasound settings, how often treatment should be repeated, or which biological markers most reliably show that it is working. Many preclinical tumor models do not fully mimic the complex, immune‑resistant nature of human glioblastoma, and safety data on normal brain tissue remain limited. The authors call for clearer reporting standards, better animal models, and broader measures of treatment response, including immune and blood vessel changes and advanced imaging.
What this could mean for future patients
In everyday terms, sonodynamic therapy is being explored as a way to “light up” tumor‑selective drugs with sound, so that only cancer cells feel the brunt of the damage while healthy brain is spared. Current evidence in animals suggests that this approach can slow tumor growth and may work well alongside surgery, chemotherapy, and possibly immunotherapy. Early patient trials are now testing whether the method is safe, how brain tissue responds, and how to fit it into existing care plans. If researchers can better understand and standardize how sound, drugs, and tumors interact, sonodynamic therapy could grow from an experimental idea into a useful extra tool against one of the most difficult brain cancers.
Citation: Özdemir, Z., Brederecke, T., Backhaus, P. et al. Preclinical evidence of sonodynamic therapy in glioblastoma and challenges towards clinical translation: a review of the literature. npj Acoust. 2, 17 (2026). https://doi.org/10.1038/s44384-026-00051-y
Keywords: glioblastoma, sonodynamic therapy, focused ultrasound, reactive oxygen species, brain cancer treatment