Clear Sky Science · en
Lifetime management of primary mitral regurgitation through integrated surgical and transcatheter reinterventions
Why this heart story matters
Many people live for years with a leaky heart valve called primary mitral regurgitation without feeling ill, yet this quiet problem can slowly stretch and weaken the heart. This article explains how doctors now think about caring for these patients not just at one operation, but across an entire lifetime, combining surgery, catheter procedures, and careful follow up to keep the valve working and options open for the future.
Understanding a leaky mitral valve
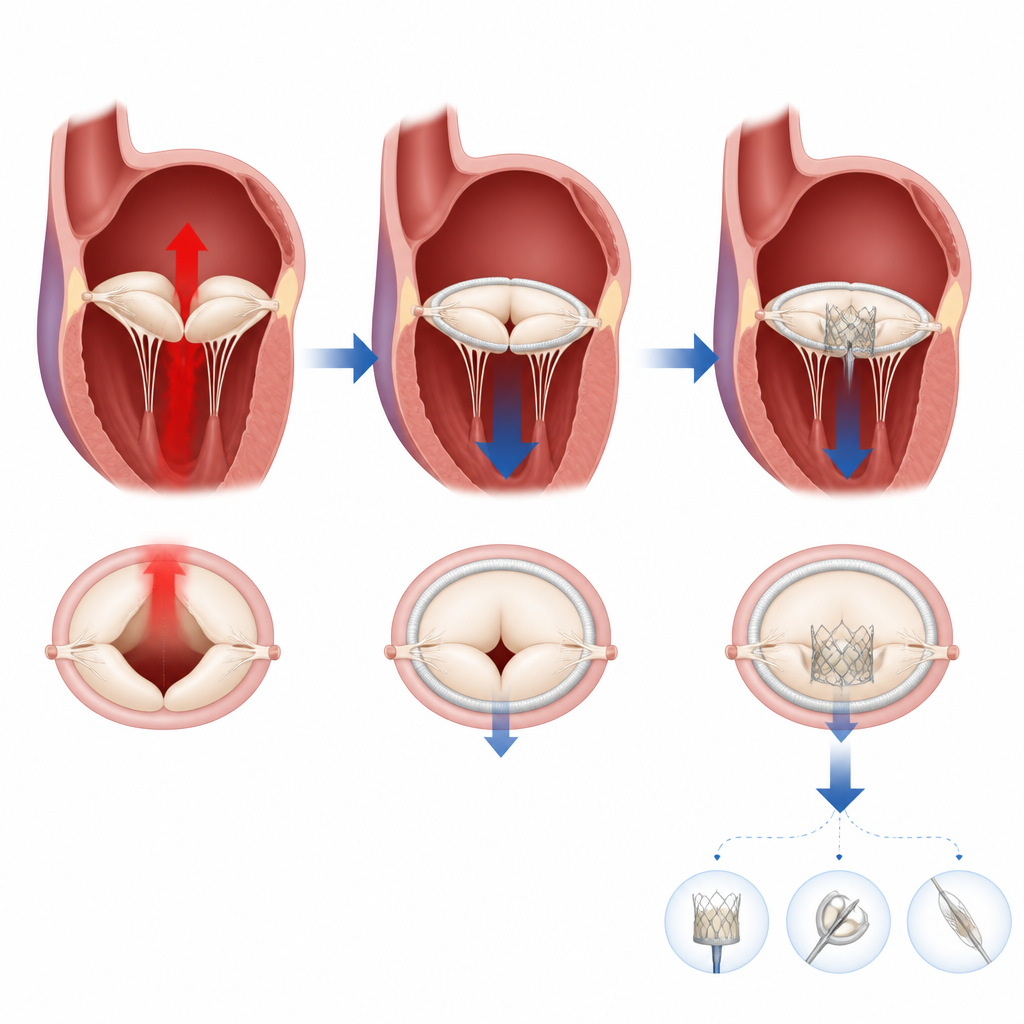
The mitral valve sits between the heart’s main pumping chamber and the upper chamber on the left side, opening and closing with every beat. In primary mitral regurgitation, the valve tissue itself is faulty, so blood spurts backward instead of all of it moving forward, forcing the heart to work harder. The review describes a range of valve types, from thin, fragile leaflets that tear to thick, floppy ones with extra tissue, and shows how modern heart scans, especially ultrasound, help doctors map each person’s unique valve shape and the severity of the leak before choosing treatment.
Acting early rather than waiting for trouble
For many years, doctors waited to operate until people with severe leakage developed shortness of breath or clear weakness of the main pumping chamber. New evidence and updated European guidelines argue for a shift toward earlier action in suitable patients, even when they feel well. When surgery is done before the heart and upper chamber stretch too much or before rhythm problems like atrial fibrillation appear, repairs are more likely to last, the valve is less likely to leak again, and long term survival approaches that of people without valve disease.
Designing repairs that last
Open heart surgery to repair the valve is the preferred first treatment for most people who can safely undergo an operation. The article explains that a sturdy supporting ring is almost always needed to keep the valve opening from stretching and to bring the leaflets together firmly. Surgeons may trim and reshape the leaflets or add artificial strings to restore smooth motion, but they must avoid making the opening too small or pushing the valve too far toward the heart’s outlet, both of which can create new blockages. Studies that have followed patients for more than a decade show that carefully done repair keeps leaks from returning in most people and that using a ring and leaving no more than a trace of leak at the end of surgery are key to long term success.
Other first steps when standard repair is not possible
Not everyone is a good candidate for classic repair. In some cases the valve is too damaged or calcified and must be replaced with a mechanical or tissue valve, each carrying trade offs between durability, blood thinner use, and the need for future procedures. Frail or very high risk patients may instead receive catheter based treatments that do not require opening the chest. One option clips the valve leaflets together to reduce leakage, while newer devices can fully replace the valve through tubes in the veins. These less invasive methods can help many people, but on average they do not last as long as surgical repair, and they can leave a tighter opening that complicates any later procedure.
Planning for the second and third procedures
A major theme of the review is that the first treatment strongly shapes what can safely be done if the valve fails again years later. If an initial repair eventually leaks, surgeons can often repair it again or replace the valve, and in high risk patients catheter techniques can sometimes be used on the repaired valve or supporting ring. When a tissue valve wears out, another valve can often be placed inside it using a catheter, avoiding another full operation, although small original valves can leave high pressure across the new one. After clipping procedures, repeat clipping or complex surgery may still be possible, but both carry higher risk than treating a valve that has never been touched. For each step, the author stresses the need for a heart team to choose options that solve today’s problem while leaving room for future fixes.
Caring for the whole person over time
Lifetime management is not only about devices and operations. The article calls for organized heart valve clinics that provide regular scans after treatment, watch for returning leaks, manage heart rhythm problems, and address blood pressure, weight, and infection prevention. In primary mitral regurgitation, timely and durable repair can restore near normal life expectancy for many, but only if it is paired with ongoing care and thoughtful planning for what might be needed decades later. In everyday terms, that means treating a leaky valve as a long journey rather than a single moment in the operating room, with a coordinated team guiding patients through each stage.
Citation: Tabata, M. Lifetime management of primary mitral regurgitation through integrated surgical and transcatheter reinterventions. npj Cardiovasc Health 3, 28 (2026). https://doi.org/10.1038/s44325-026-00129-2
Keywords: primary mitral regurgitation, mitral valve repair, transcatheter mitral procedures, valve reintervention, heart team care