Clear Sky Science · en
Enabling ankle-brachial index prediction from doppler sounds using deep learning
Why blood flow in the legs matters
Millions of people worldwide live with poor blood flow to their legs, a condition called peripheral artery disease. When leg arteries narrow or harden, walking can become painful and wounds may not heal, sometimes leading to amputation. Doctors have a simple test, the ankle-brachial index, that compares blood pressure at the ankle and the arm to spot trouble early. But this test is slow, needs special equipment, and often fails in people whose leg arteries are too stiff to squeeze—especially those with diabetes or kidney disease. This study explores whether a computer can listen to the familiar whooshing sounds from a handheld Doppler device and instantly judge how well blood is reaching the foot.
From whooshing sounds to a risk score
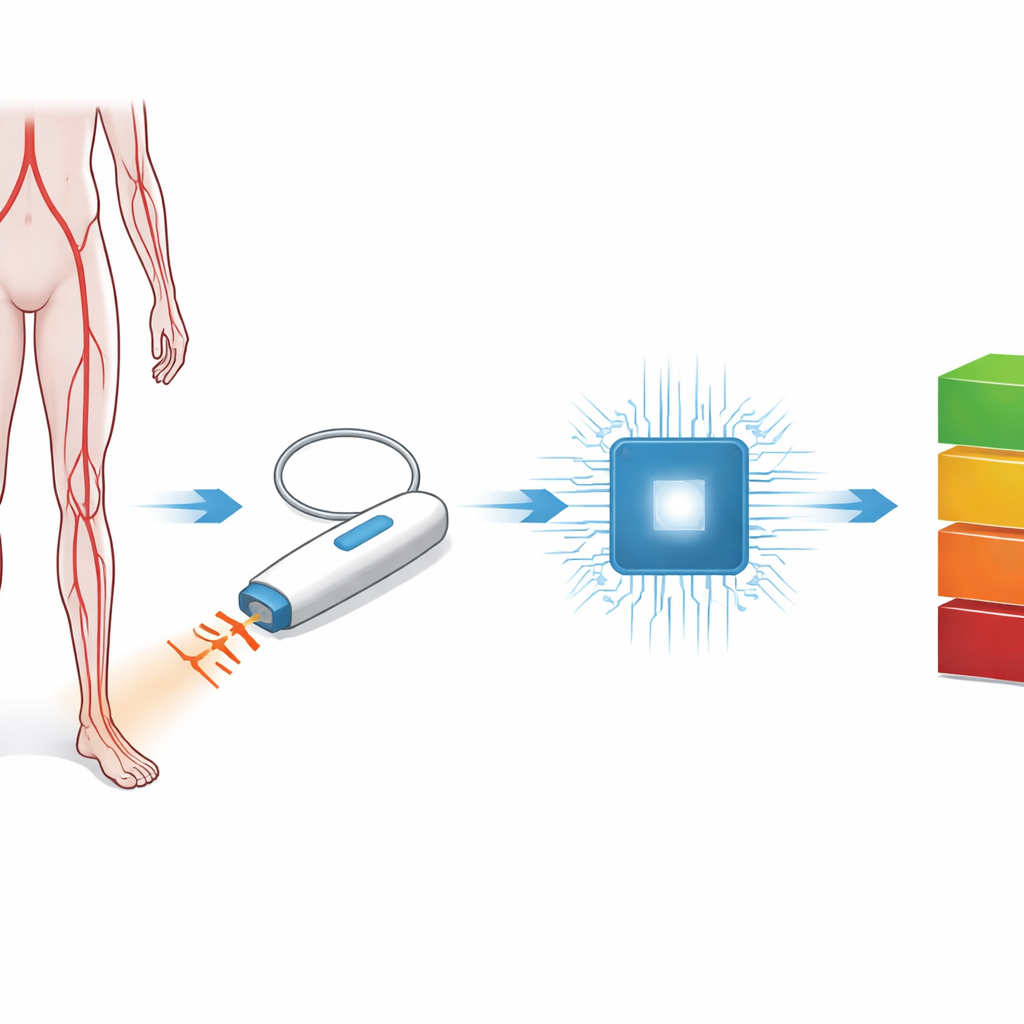
The researchers created a system they call AutoABI. Instead of wrapping multiple blood pressure cuffs around a patient’s limbs, a clinician uses a standard handheld Doppler probe at the ankle, just as they already do in everyday practice. The probe picks up the sound of blood pulsing through the artery. These sounds were recorded in short four-second clips from nearly 800 tests in 198 patients referred to a hospital vascular lab for concerns such as leg artery disease or diabetes-related circulation problems. The goal was to see whether a computer program could sort each recording into one of four ankle-brachial index ranges, from very poor blood flow to clearly normal.
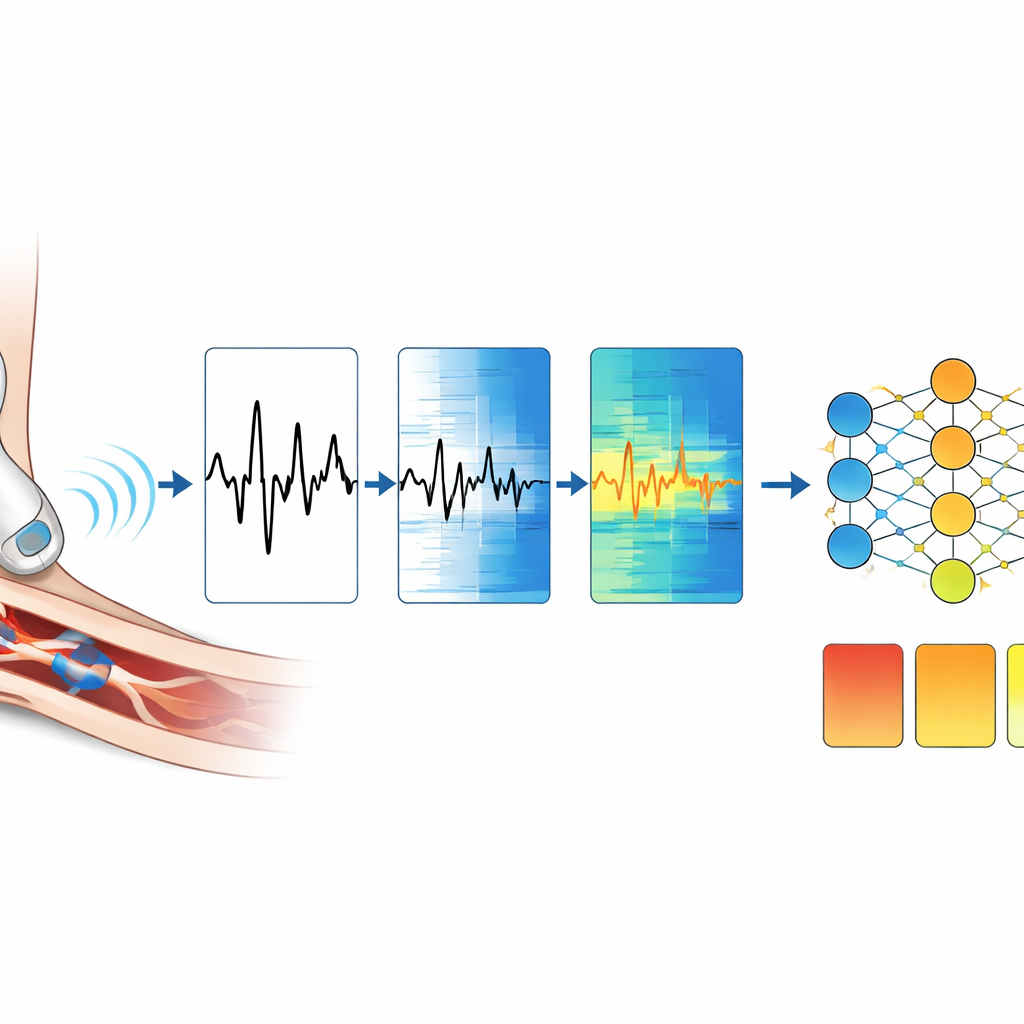
Teaching a computer to listen like a specialist
To make the audio understandable to a computer, the team first broke each recording into one‑second snippets that captured individual heartbeats. They then converted each snippet into a colorful picture called a spectrogram, which shows how the sound’s energy changes over time and frequency. These pictures were fed into deep learning models known as convolutional neural networks. The models, built on two versions of a common image-analysis design called ResNet, learned to recognize patterns in the Doppler sounds that match clinically important ankle-brachial index categories. The researchers carefully split the data so that sounds from the same patient never appeared in both training and testing, helping ensure that the system learned general rules rather than memorizing specific cases.
How well the system performed
Once trained, AutoABI showed strong ability to distinguish between the four blood-flow categories. For both model versions, it correctly separated normal circulation from disease with very high accuracy, measured using standard statistics such as the area under the receiver operating characteristic curve, which approached or exceeded 0.95 for all classes. Most mistakes occurred at the fuzzy borders between “almost normal” and mildly reduced blood flow, where even human experts can disagree by eye or ear. Importantly, when the team applied the system to a small group of diabetic patients whose leg arteries were too stiff for conventional ankle-brachial index measurement, the model’s predictions matched expert expectations based on the shape of the Doppler waveforms in all ten cases.
What this could mean in the clinic
The authors compared their approach to commercial automated ankle-brachial index machines that still rely on multiple cuffs and pressure readings. Those devices are fast but share the same weakness: they do not work well when arteries are rigid and cannot be compressed. AutoABI, by contrast, needs only the widely available handheld Doppler and a device capable of running the deep learning model, such as a smartphone. It trades exact numerical values for broader ranges, but in return it can provide rapid, objective guidance at the bedside, in emergency rooms, or in clinics that lack a full vascular lab. The system could be especially useful in resource-limited settings and for high‑risk patients where traditional measurements are unreliable.
Next steps toward real-world use
The study is an early proof of concept, and the authors emphasize its limits. The dataset, while carefully collected, was modest in size, and the number of non-compressible vessels studied was very small. The quality of the recordings depended on how the technologist held the probe and on background noise, and the system has not yet been tested across different brands of Doppler machines or in busy outpatient environments. Future work will need larger, more diverse patient groups, inclusion of medical history, and ongoing monitoring to guard against bias and performance drift. Still, the results suggest that teaching computers to “listen” to blood flow could make leg circulation testing faster, cheaper, and more widely available—potentially catching serious vascular disease before it leads to life‑changing complications.
Citation: Rao, A., Battenfield, K., Fereydooni, A. et al. Enabling ankle-brachial index prediction from doppler sounds using deep learning. npj Cardiovasc Health 3, 21 (2026). https://doi.org/10.1038/s44325-026-00116-7
Keywords: peripheral artery disease, ankle-brachial index, Doppler ultrasound, deep learning, limb perfusion