Clear Sky Science · en
Phenotypic convergence and collateral susceptibility development in Pseudomonas aeruginosa under antibiotic exposure in ICU patients
Why mixing antibiotics in the ICU matters
When people in intensive care develop lung infections, doctors often reach for powerful combinations of antibiotics to save their lives. But the same drugs that knock back deadly germs can also drive them to evolve, sometimes into harder-to-treat forms. This study asks a pressing question: can the way we shuffle different antibiotics in real ICU patients actually tilt evolution in our favor, making dangerous bacteria more vulnerable again?
The threat lurking in ventilators
One of the main culprits in ventilator-associated pneumonia is Pseudomonas aeruginosa, a highly adaptable bacterium that thrives in hospitals and often resists multiple drugs. ICU patients on breathing machines are especially exposed: their lungs can harbor large bacterial populations that quickly adapt to whatever antibiotics they encounter. Because treatment decisions change rapidly with a patient’s condition, these patients offer a natural experiment in how real-world antibiotic use shapes bacterial evolution.
Following bacteria through a patient’s stay
Researchers tracked 25 ICU patients who were colonized or infected with the same strain of P. aeruginosa over time. These patients typically received several different antibiotic classes over weeks of treatment. From repeated respiratory samples, the team measured how drug susceptibility changed and sequenced the bacteria’s DNA to see which mutations appeared. They compared these clinical findings with controlled lab experiments, where two well-known P. aeruginosa strains were exposed repeatedly to single antibiotics, forcing them to adapt step by step.
When resistance comes with hidden weaknesses
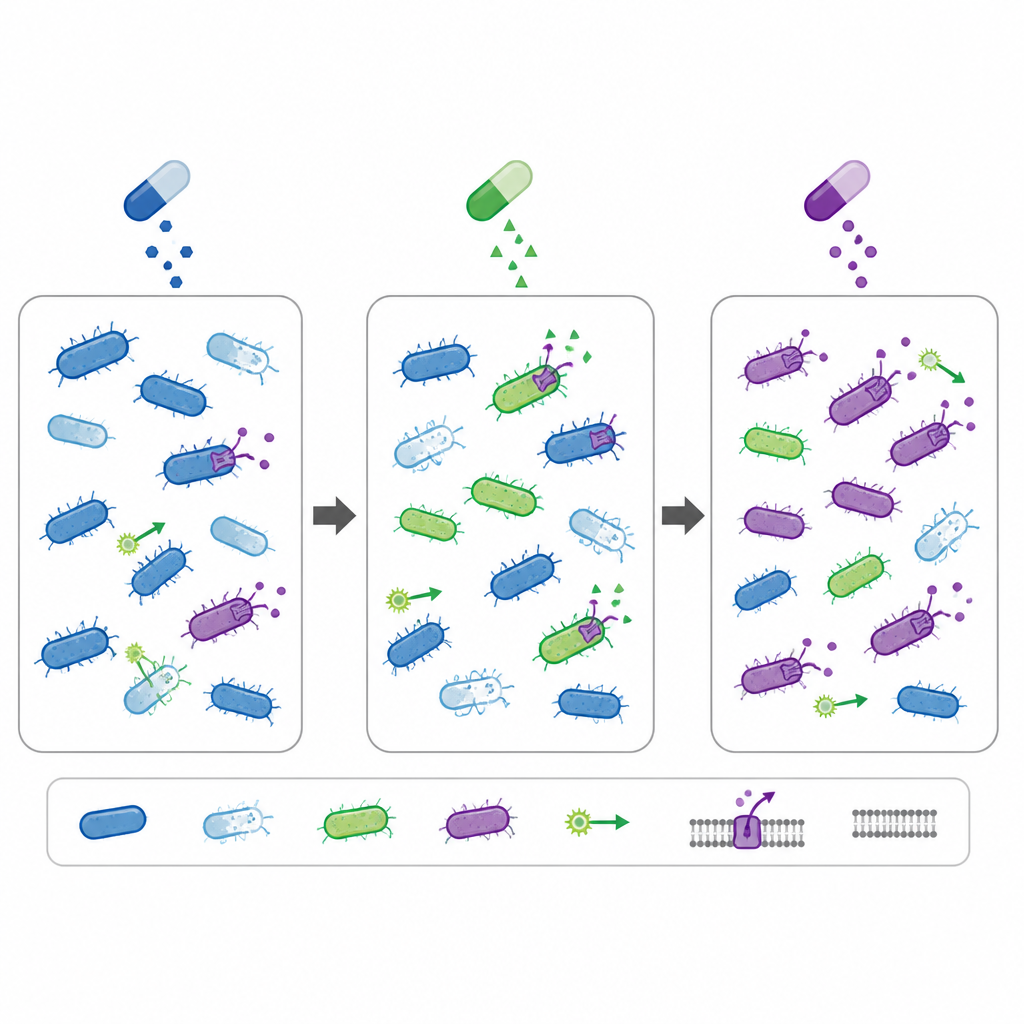
In both patients and lab cultures, prolonged exposure to a single antibiotic, such as ciprofloxacin or imipenem, often led to resistance. This was linked to well-known changes in bacterial targets and in pumps that expel drugs from the cell. But these adaptations came at a cost. As bacteria evolved resistance to one drug, they sometimes became more sensitive to others, a trade-off called collateral susceptibility. In ICU patients, the number of different antibiotic classes given did not strongly increase resistance to those drugs, but was linked to lower resistance against drugs the patients had not actually received, hinting that switching between classes can create exploitable weak spots.
Zooming in on bacterial evolution in the lab
In the lab, bacteria were subjected to slowly increasing doses of four common anti-Pseudomonas drugs over 20 rounds of exposure. The strains quickly became highly resistant, in some cases tolerating hundreds of times the initial drug level. Genetic analysis showed complex “family trees” of mutations, with some changes sweeping through almost the entire population, while others arose only in subgroups. Different antibiotics drove different evolutionary paths, yet the end result often converged on similar resistance patterns and similar collateral changes in sensitivity to other drugs. Some mutations also altered features like surface sugars and movement, sometimes reducing growth but increasing cell-killing ability.
What this means for treating the sickest patients
Taken together, the patient data and lab experiments suggest that using multiple antibiotic classes in sequence may do more than simply broaden coverage. It can push P. aeruginosa into evolutionary trade-offs that make it less fit against other drugs, dampening the rise and persistence of highly resistant strains. For lay readers, the key message is that how we combine and switch antibiotics can subtly steer bacterial evolution. Rather than always driving resistance in one direction, thoughtful multi-drug use in the ICU might help create new treatment openings, making some tough bacteria more treatable again and offering a potential tool to slow the march of multidrug resistance.
Citation: van der Schalk, T.E., Berkell, M., Hottebeekx, A. et al. Phenotypic convergence and collateral susceptibility development in Pseudomonas aeruginosa under antibiotic exposure in ICU patients. npj Antimicrob Resist 4, 38 (2026). https://doi.org/10.1038/s44259-026-00199-3
Keywords: antibiotic resistance, collateral susceptibility, Pseudomonas aeruginosa, ICU infections, combination therapy