Clear Sky Science · en
Host factors, inflammatory markers, and clinical outcomes of Naegleria fowleri meningoencephalitis
A deadly waterborne threat in a warming world
Most people think of warm lakes and rivers as places for play or prayer, not as sources of a rare brain infection. Yet Naegleria fowleri, sometimes called the brain eating amoeba, lives in such waters and can cause a fast moving and often fatal disease when water is forced high into the nose. This study follows the largest known outbreak of this infection, in the Indian state of Kerala in 2025, to ask a simple but urgent question: who survives, who does not, and why, in an age of rising temperatures and changing water use?
What happened during the Kerala outbreak
In 2025, Kerala recorded 200 confirmed cases of primary amoebic meningoencephalitis, the brain infection caused by Naegleria fowleri. Past reports suggested that more than 97 percent of patients die, but here the death rate among patients with known outcomes was about 45 percent. All patients were treated using the same drug plan based on amphotericin B, sometimes combined with miltefosine, and many received intensive care. Cases first appeared sporadically early in the year, then surged from August through November, during and after the monsoon, when warm, often stagnant water is common. People had been exposed not only in rivers and ponds but also through piped and well water used in homes. 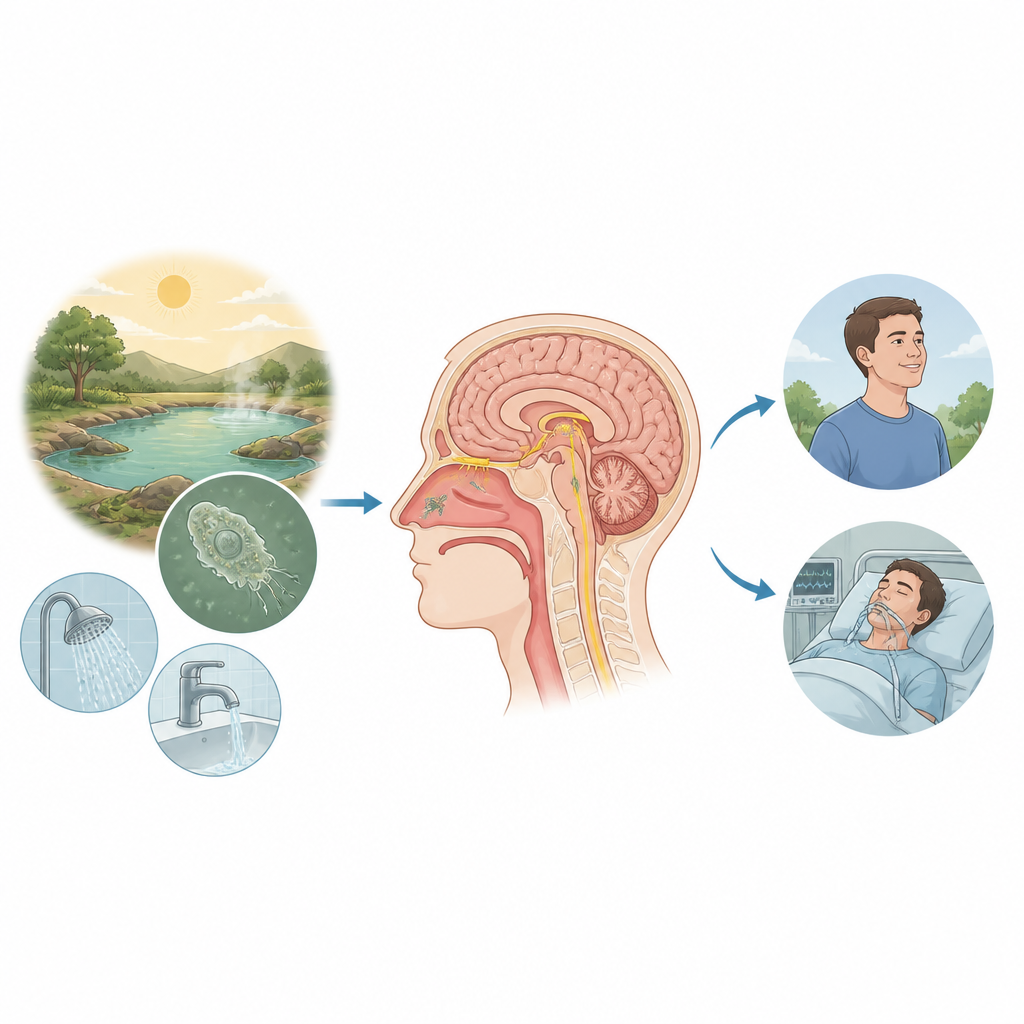
Who was most at risk
The researchers collected detailed information on age, health history, water exposure, timing of symptoms and treatment, and the need for breathing machines. They then used statistical models to see which factors were linked to death. One health condition clearly stood out: diabetes. Patients with diabetes were roughly two to three times more likely to die than those without it, even after accounting for age, sex, illness severity, and treatment timing. This pattern remained stable across multiple checks of the data. Asthma, in contrast, appeared to be linked with better survival in simple comparisons, but that signal weakened when other factors were considered, so it is treated as an open question rather than a firm finding.
Why inflammation did not tell the story
Because many severe infections can be tracked using blood markers of inflammation, the team measured several such markers, including well known signaling molecules in the blood and a simple blood count ratio called the neutrophil to lymphocyte ratio. These values were high across the board, showing that patients were very sick, but they did not differ meaningfully between those who lived and those who died. The amount of amoeba genetic material found in spinal fluid also failed to predict outcome directly, even though higher amounts did match up with worse brain function at the time of hospital arrival. Together, these findings point toward a grim idea: much of the brain damage may occur very early, before patients reach care, so later inflammation levels do not change the final outcome very much.
The importance of speed and support
The timing of treatment still seemed to matter. Patients who started the drug plan within two days of their first symptoms had a lower death rate than those treated later, hinting at a narrow window in which medicines and intensive support can change the course of illness. Mechanical ventilation, used to support breathing, also showed a trend toward better survival, reinforcing the value of aggressive care once the disease is suspected. Yet even the best model the authors built explained only a small share of the differences in who survived, suggesting that hidden factors, such as subtle immune traits or differences among amoeba strains, may also shape the outcome. 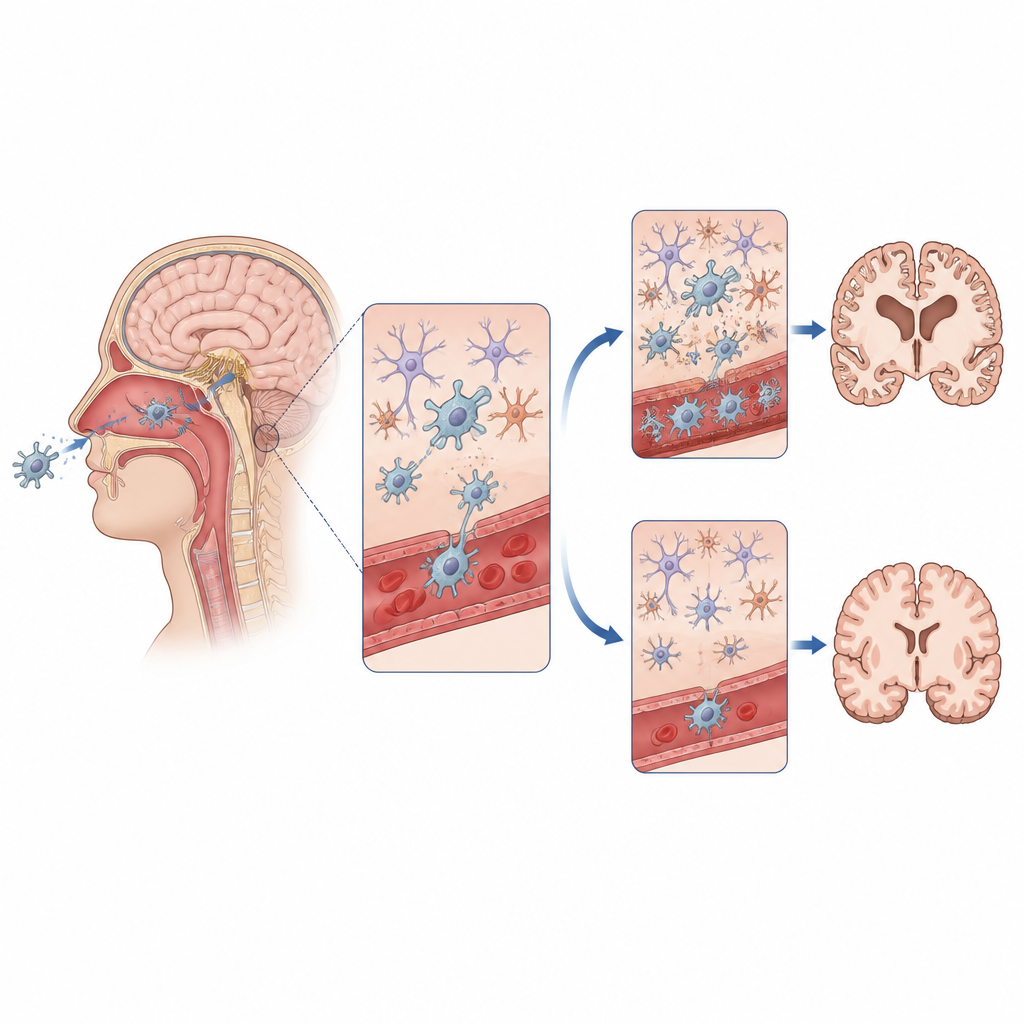
What this means for patients and public health
For a disease long regarded as almost uniformly fatal, the Kerala outbreak offers cautious hope and a clear warning. Standardised treatment and strong critical care can greatly reduce the death rate, but diabetes appears to make patients especially vulnerable, and usual blood tests offer little help in guessing who will live. As climate change warms freshwater and expands the range of Naegleria fowleri, more communities may face similar outbreaks. The study suggests that rapid recognition, very early treatment, protection of household water supplies, and special attention to people with diabetes will be crucial for turning a once hopeless infection into one that more patients can survive.
Citation: Kadukkatti, V., Mathew, B.K. & Asaga, P.M. Host factors, inflammatory markers, and clinical outcomes of Naegleria fowleri meningoencephalitis. Commun Med 6, 290 (2026). https://doi.org/10.1038/s43856-026-01658-8
Keywords: Naegleria fowleri, primary amoebic meningoencephalitis, diabetes and infection, waterborne brain infection, climate change and disease