Clear Sky Science · en
Monitoring viral evolution and epidemiological characteristics of SARS-CoV-2 during 2022–2023 using Integrated Genomic Surveillance
Why watching this virus still matters
Even after the emergency phase of COVID-19 ended, the virus that causes it, SARS-CoV-2, continues to change. New versions can spread faster, slip past immune protection, or affect some age groups more than others. This study from Germany shows how combining virus genetics, case records, and laboratory experiments can spot such shifts early and guide public health decisions in a calmer, post-crisis world. 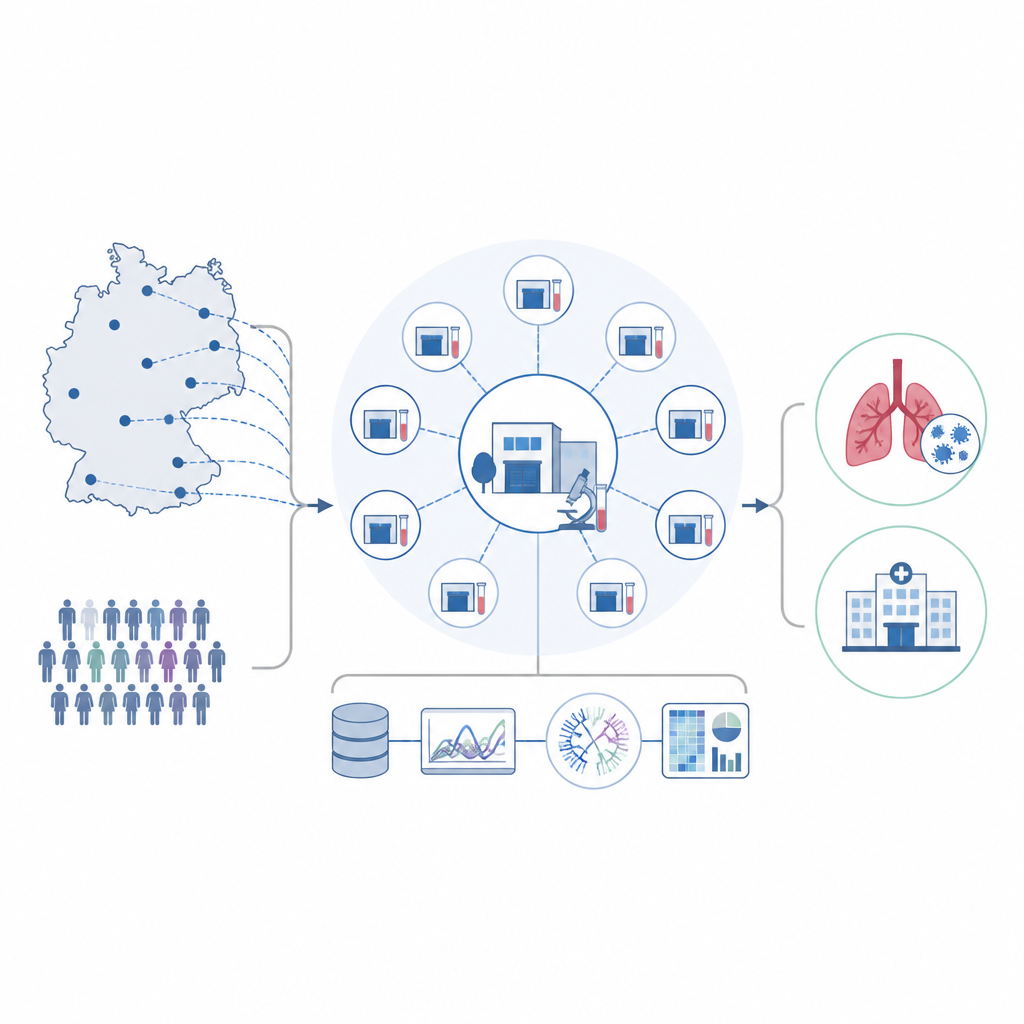
Tracking changes across the country
The researchers built a nationwide network of diagnostic laboratories that send a small, randomly chosen set of positive COVID-19 samples each week to the Robert Koch Institute for whole-genome sequencing. Between December 2021 and April 2023 they decoded 4,595 viral genomes from 24 labs spread across 14 of Germany’s 16 federal states. They compared this lean, continuous stream of data with a much larger, short-term sequencing effort that had produced over half a million genomes. The patterns of variants over time matched closely, showing that a carefully designed, smaller system can still provide an accurate picture of how the virus is evolving.
What the shifting variants looked like
The sequence data revealed a rapid handover from the Delta variant in late 2021 to a series of Omicron offshoots. First came BA.1 and BA.2, which took over by early 2022, followed by BA.5 and its descendants such as BQ.1, and later by recombinant XBB lineages that combine pieces of earlier Omicron strains. By March 2023, XBB versions made up the majority of the viruses detected. The study also showed that Omicron did not just change its genetic code at random; key changes clustered in the spike protein, the part of the virus that attaches to human cells and is the main target of antibodies.
Who got sick and how badly
The team linked 516,128 sequenced viruses with individual case records from Germany’s mandatory COVID-19 notification system, then focused on 84,639 people infected with major Omicron lineages. They found that early Omicron waves, BA.1 and BA.2, were relatively more common in children, especially those under 15, compared with later variants. Men were less often reported as infected but had a higher chance of being hospitalized once infected. Using statistical models that accounted for age, sex, variant, and calendar month, the strongest predictors of hospitalization were being male and being older, particularly above 60 years. Apparent differences in hospitalization risk between later variants mostly disappeared once changes in testing habits and reporting over time were taken into account.
What the virus did inside human airway cells
To move beyond population patterns, the scientists grew human nasal, bronchial, and alveolar (deep lung) cell layers at an air–liquid interface, which mimics the surface of the breathing passages. They infected these cultures with an early pandemic virus, Delta, and several Omicron sublineages. All Omicron versions tested were much harder for pre-Omicron antibodies to neutralize, showing strong immune escape. In nasal and bronchial cells, Omicron variants such as BQ.1.1 and XBB.1.9.2 multiplied faster in the first hours after infection than the early virus, hinting at efficient spread through the upper airways, although their peak levels later on could be lower. In deep lung cells, most Omicron variants grew less well than the original virus and Delta, but XBB.1.9.2 was a notable exception, reaching higher early levels and showing the steepest growth, suggesting it may retain some capacity to affect the lower lungs. 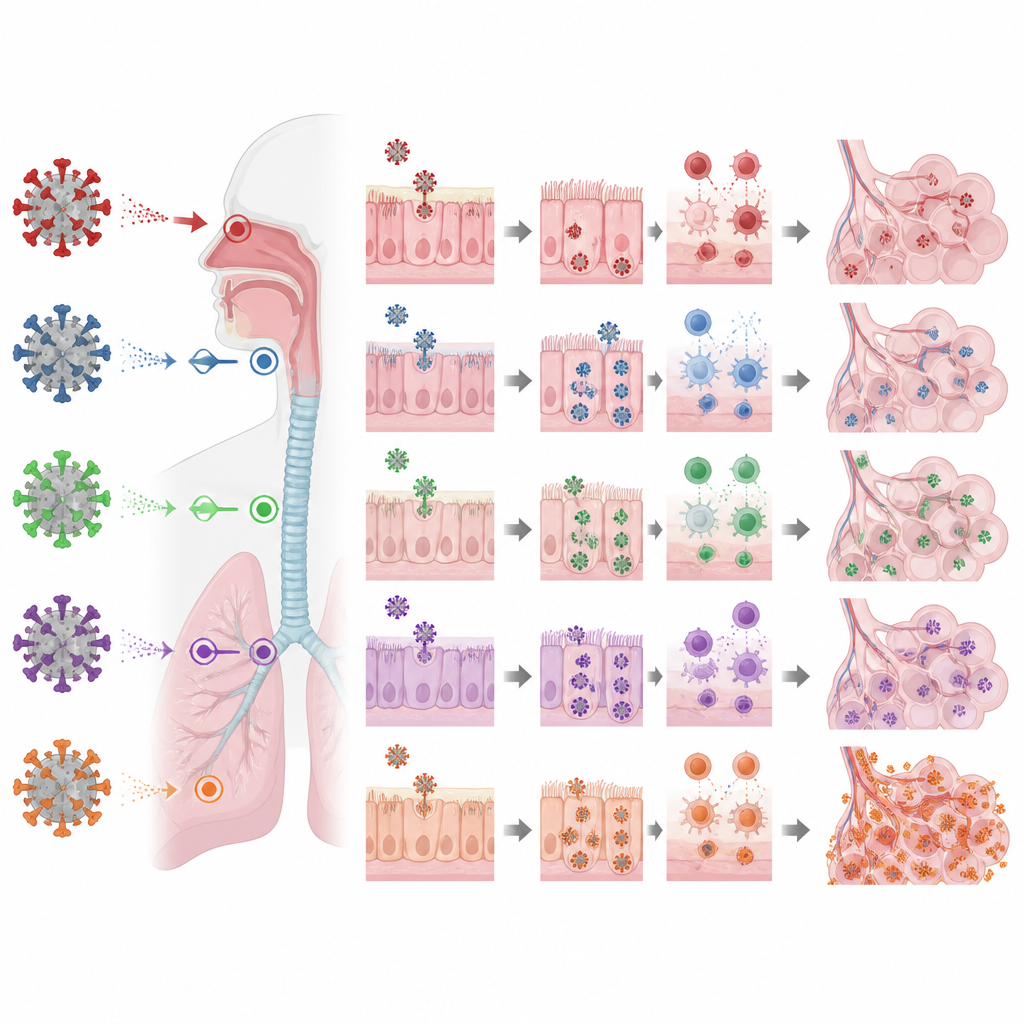
Signals from the immune response
The team also measured molecules called interferons, which are part of the body’s first-line antiviral alarm system. In upper airway cells, Omicron variants triggered strong type I and type III interferon responses after a delay, with BQ.1.1 standing out for particularly high levels. Such responses in the nose and bronchi are thought to help limit disease severity. In contrast, in deep lung cell cultures the original virus and Delta produced the strongest interferon signals, while Omicron variants triggered weaker responses, again with XBB.1.9.2 at the higher end among Omicron strains.
What this means for living with COVID-19
Overall, the study paints a picture of a virus that is still adapting to humans, favoring quick growth in the upper airways, strong escape from existing antibodies, and varied behavior in the lungs. By tying together nationwide sequencing, case data, and realistic lab models of the human respiratory tract, the German network shows how countries can keep watch for new variants in a sustainable way. Such integrated surveillance can detect changes in spread, age patterns, and viral behavior early on, helping health authorities respond promptly without the extraordinary resources used in the first years of the pandemic.
Citation: Mache, C., Kerber, R., Schulze, J. et al. Monitoring viral evolution and epidemiological characteristics of SARS-CoV-2 during 2022–2023 using Integrated Genomic Surveillance. Commun Med 6, 305 (2026). https://doi.org/10.1038/s43856-026-01647-x
Keywords: SARS-CoV-2 variants, genomic surveillance, Omicron evolution, respiratory cell models, COVID-19 epidemiology