Clear Sky Science · en
Genetic drivers of congenital cardiac fibrosis
Why heart scarring in children matters
Many babies are born with structural heart problems, known as congenital heart disease, and more of them now survive into adulthood thanks to better surgery and care. Yet a hidden threat remains inside their hearts: scar-like tissue called fibrosis. This review explains how genes that guide early heart formation, especially those controlling tiny cell structures called cilia, may also shape who develops harmful scarring and who does not. Understanding these genetic drivers could one day help doctors spot high-risk patients early and design treatments that slow or prevent the buildup of stiff tissue that weakens the heart.
How heart support cells shape a growing heart
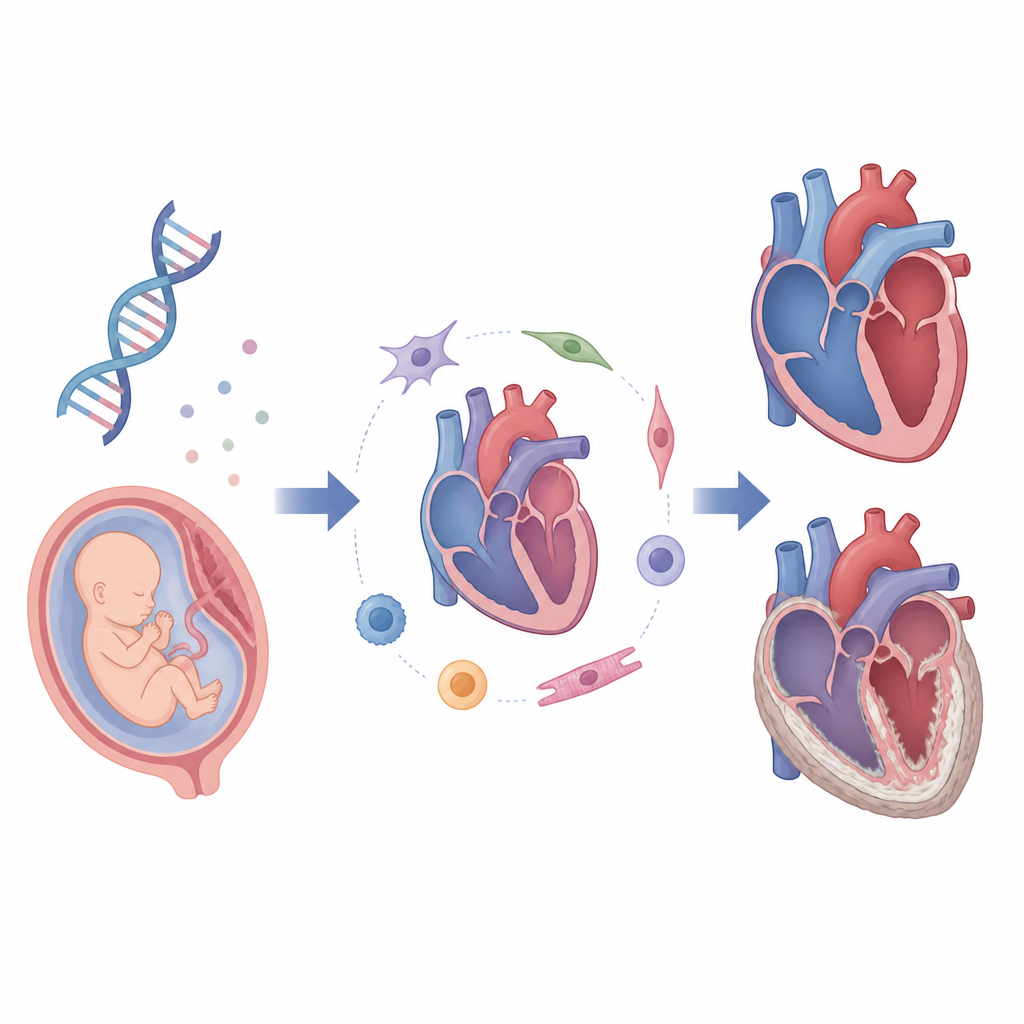
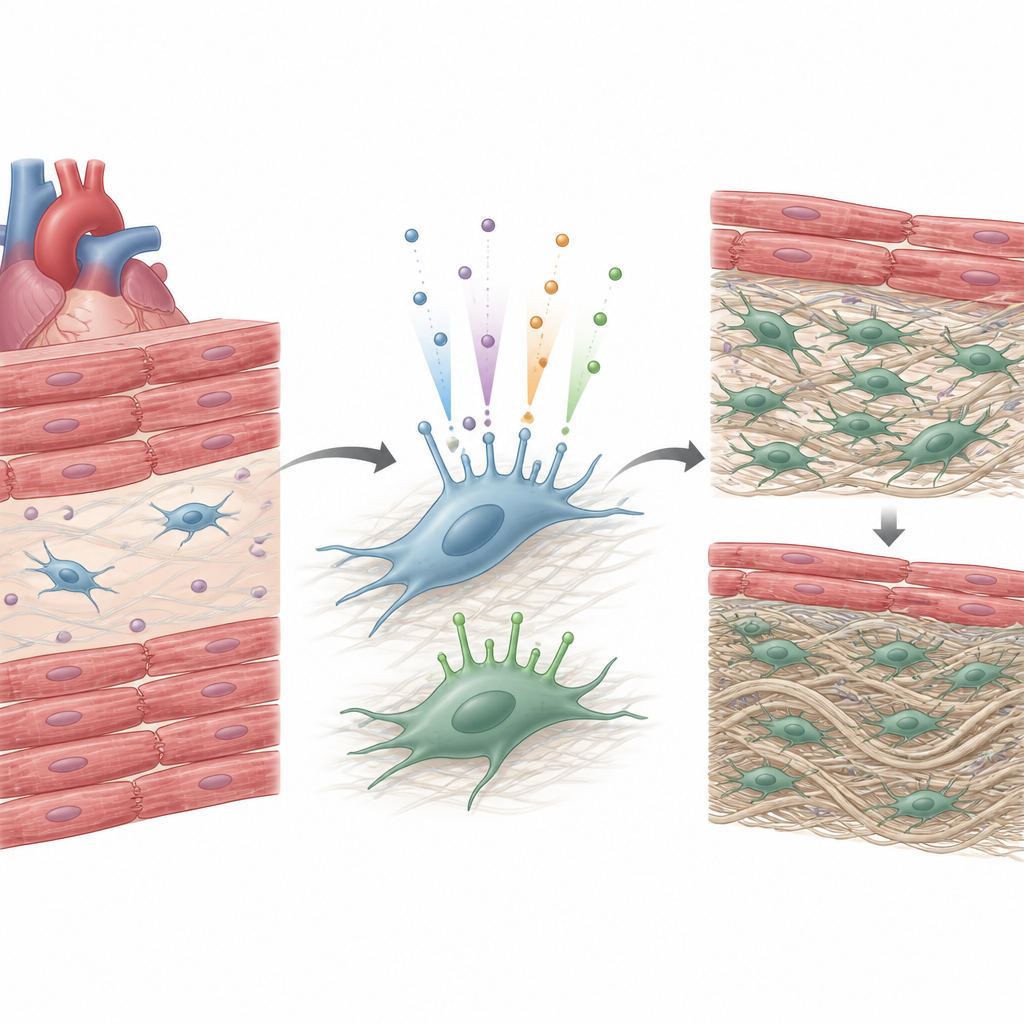
The heart is one of the first organs to form in the embryo, assembling from several cell populations that fold and connect to create chambers, valves, and large vessels. Alongside the muscle cells that pump blood are fibroblasts, support cells that build and maintain the heart’s scaffolding made of collagen and other proteins. During development, fibroblasts arise from the heart’s outer layer, its inner lining, and migrating nerve-related cells through shape-changing processes. They first help the heart grow by promoting muscle cell division and alignment, then gradually shift toward producing the mature matrix that makes the heart strong enough to handle rising blood pressure.
Tiny cellular antennas with big effects
Many heart cells, including fibroblasts, carry cilia, hair-like projections that act as miniature antennas for chemical and mechanical signals. These structures sense fluid flow, guide left-right orientation of the body, and help cells respond to cues that tell them when to move, divide, or change identity. The review shows that genes needed to build and operate cilia also steer key signaling pathways involved in heart shaping and in turning quiet fibroblasts into active scar-forming cells. Mutations in cilia-related genes are already known to cause complex heart malformations, and evidence from animal models and rare human cases suggests they may also tilt the balance toward excessive matrix buildup and valve or wall thickening.
Why some heart defects scar more than others
Not all congenital heart problems lead to the same scarring pattern. The authors describe distinct forms, including a rind of elastin-rich tissue lining the inside of the left heart in hypoplastic left heart syndrome, patchy replacement of dead muscle by stiff tissue in cardiomyopathies, and more diffuse thickening between muscle fibers in repaired valve and vessel defects. These patterns arise from a mix of inherited variants, altered gene activity, and environmental stresses such as abnormal pressure, low oxygen, or surgical injury. Certain conditions, such as trisomy 21, cilia disorders, and maternal diabetes, appear to increase both the chance of being born with a heart defect and the likelihood that fibroblasts will overreact and deposit excess matrix.
New tools to connect genes with scarring
The review highlights a wave of technologies that can finally tackle the genetic roots of heart fibrosis in children. Single-cell RNA sequencing can read thousands of genes in individual heart cells, revealing specialized fibroblast subtypes and how their programs change in different defects. Patient-derived stem cells can be turned into miniature heart tissues, where researchers can watch how specific mutations alter communication between support cells, muscle cells, and blood vessel cells. Advanced cardiac imaging and blood markers now measure fibrosis in living patients, while large genetic studies and network-based computer models can sift through many variants at once to identify interacting pathways that drive scarring.
What this means for patients and families
Overall, the article argues that harmful heart scarring in congenital heart disease is not an inevitable byproduct of surgery or abnormal anatomy, but the result of a complex dialogue between genes, cell behavior, and mechanical stress. Cilia-centered signaling and fibroblast control pathways emerge as key hubs where multiple risk factors converge. As clinical imaging, stem cell models, and big-data genetics continue to advance, they should allow doctors to better predict which children with heart defects are likely to develop fibrosis and to test therapies that keep fibroblasts in a healthier, less scarring state. For patients and families, this raises the possibility of more personalized care that preserves heart function over a lifetime.
Citation: Zeigler, A.C., Touma, M. Genetic drivers of congenital cardiac fibrosis. Commun Biol 9, 722 (2026). https://doi.org/10.1038/s42003-026-10353-2
Keywords: congenital heart disease, cardiac fibrosis, cilia, cardiac fibroblasts, heart development