Clear Sky Science · en
Evolutionary digital twin framework for optimal aminoglycoside dosing in neonates with suspected sepsis
Why tiny patients and big data meet
When newborn babies develop serious infections, doctors often have only hours to start the right antibiotics in the right dose. But every baby in intensive care is different, especially preterm infants whose organs are still maturing. This study shows how a virtual "digital twin" of each baby can test antibiotic plans on a computer first, helping doctors choose doses that fight infection, protect fragile kidneys, and slow the rise of drug resistant bacteria.
Making a virtual copy of a newborn
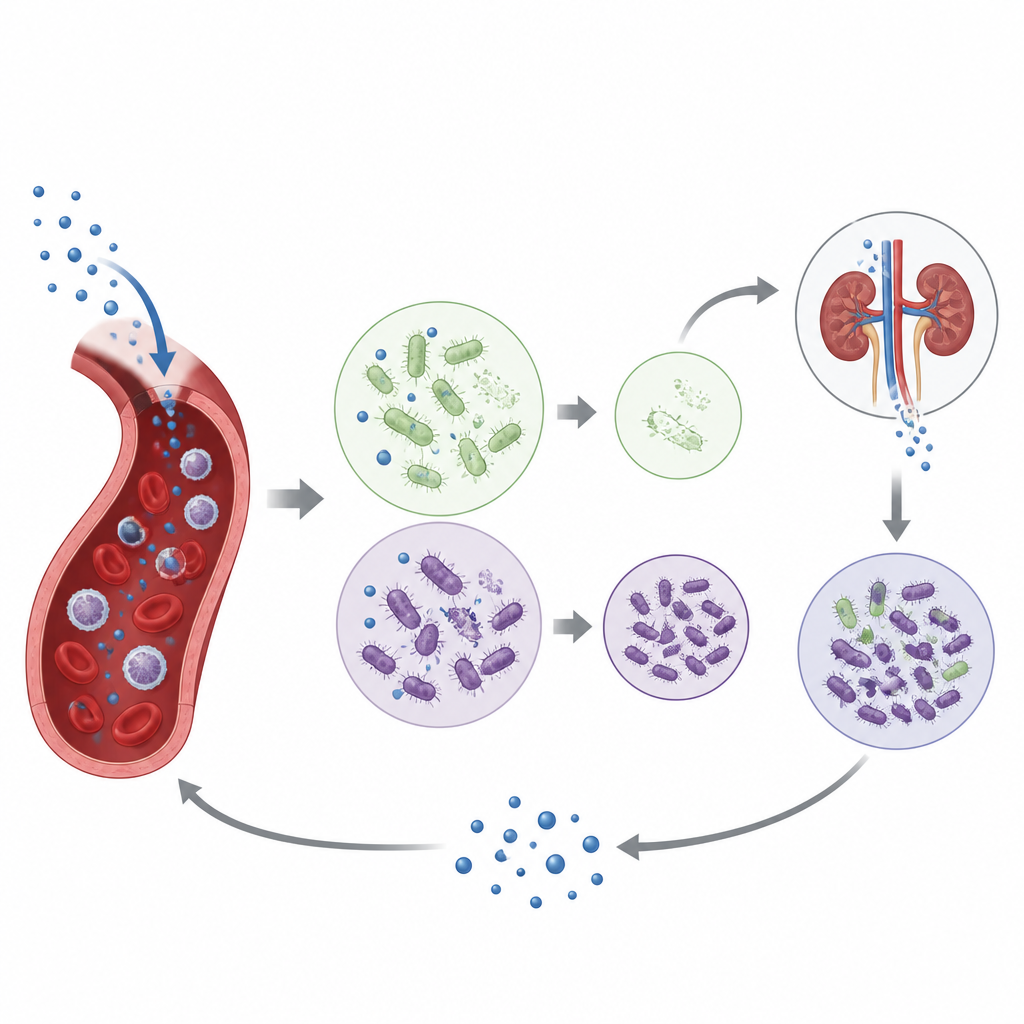
The researchers built a mathematical stand in for each baby that mimics how an aminoglycoside antibiotic, amikacin, moves through the body and affects germs. One part of the twin represents blood flow, the kidneys, and the rest of the body, predicting how the drug is distributed and cleared over time. Another part represents communities of bacteria, split into drug sensitive and more stubborn groups, and tracks how they live, compete, and die under changing drug levels. These two parts are linked, so that the virtual baby and its virtual infection evolve together during treatment.
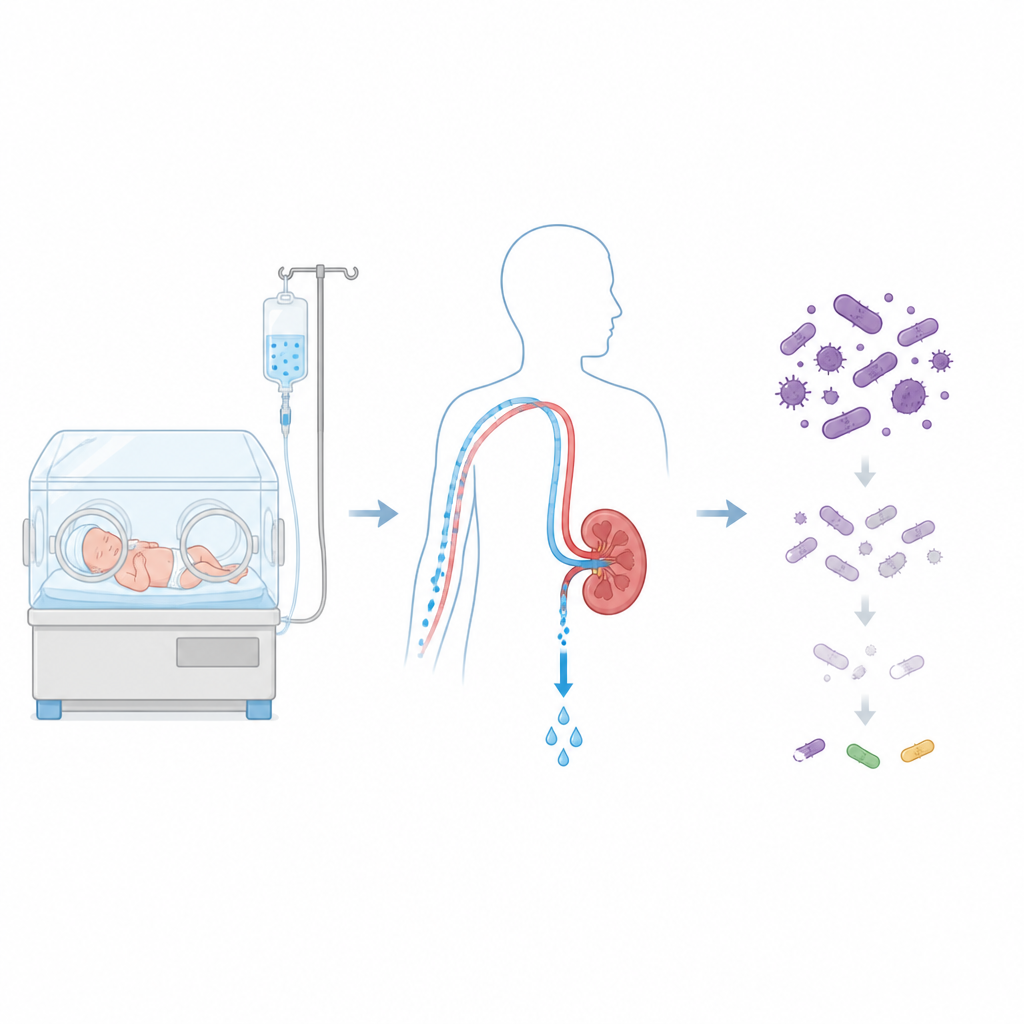
Teaching the twin to follow real kidneys
In sick newborns, kidney function can change from day to day, especially when they are extremely premature, have birth related oxygen loss, or receive other kidney stressing medicines. The team trained a type of deep learning model, called a long short term memory network, on more than 7000 real measurements of a waste product in the blood known as serum creatinine. This allowed the twin to update a key kidney filter value every day from simple bedside data. Compared with an earlier, hand built kidney model, the new approach predicted creatinine more accurately across different hospitals and disease types, giving more reliable drug level forecasts.
Checking the twin against real drug levels and infections
To make sure the twins behaved realistically, the scientists fed them real treatment records from over 1600 newborns who had received amikacin. The virtual models reproduced thousands of measured drug concentrations in the blood with modest error, even in babies receiving cooling therapy after asphyxia or extra heart support drugs. When the team looked at the model’s predicted bacterial counts, these matched whether blood cultures from the same babies were positive or negative. This suggested the twin could not only follow drug levels, but also capture the broad pattern of infection control seen in the clinic.
Letting the computer adjust the treatment
Once validated, the digital twins were used to explore treatment choices in a large virtual population covering a wide range of gestational and postnatal ages. An optimization program searched within standard dosing limits to find a personal plan for each twin that kept peak drug levels high enough to curb bacteria while letting levels fall low enough between doses to reduce kidney risk. The model also allowed the bacteria’s drug sensitivity to drift upward during therapy, imitating the slow rise of resistance. A more advanced version of the controller looked several doses ahead and adjusted schedules to prevent the late rebound of hardier bacteria, improving long term control without pushing drug levels into dangerous territory.
What this means for fragile newborns
For both simulated babies and real hospital cohorts, digital twin guided dosing schedules provided better predicted infection clearance and less expansion of resistant germs than the standard dosing rules now in use, while keeping exposure within accepted safety margins. The approach relies only on routinely collected bedside information, such as age, weight, creatinine tests, and treatment history. Although it still needs prospective testing, the work points toward a future where each newborn’s antibiotic course is continuously reshaped by a virtual companion, helping clinicians give enough drug to cure the infection but not so much that it harms the baby or fuels resistance.
Citation: Prunella, M., Romano, C., Borri, A. et al. Evolutionary digital twin framework for optimal aminoglycoside dosing in neonates with suspected sepsis. npj Digit. Med. 9, 367 (2026). https://doi.org/10.1038/s41746-026-02558-w
Keywords: neonatal sepsis, digital twin, amikacin dosing, antibiotic resistance, precision medicine